ISSN: 3080-1427 (online) / 3080-1419 (print)
Volume 1, Issue 3 (July 2025 – September 2025), pp: 1-5
![]()
Surgical Excision of Huge Recurrent Parotid Carcinoma and Reconstruction Using Supraclavicular Artery Island Flap:
A Case Report
Shadi Awny 1,a, Ahmad M Eid 1,b, Doaa Khedr 2,c, Fatma El-Husseiny 3,d, Mona Gad 2,e, Manar Mansour 2,f, Hadeel G Elghamery 4,g, Mohamed A Elbanna 1,h, Omar Hamdy 1,i *
1 Surgical Oncology Department, Mansoura University Oncology Centre, Egypt.
2 Diagnostic and Interventional Radiology Department, Faculty of Medicine, Mansoura University, Egypt.
3 Pathology Department, Faculty of Medicine, Mansoura University, Egypt.
4 Clinical Oncology and Nuclear Medicine Department, Faculty of Medicine, Mansoura University, Egypt.
E-mail:
shadiawny@mans.edu.eg a, ahmedeid_43@mans.edu.eg b, doaakhedr@mans.edu.eg c,
fatmaelhusseiny@yahoo.com d, mona_gad92@mans.edu.eg e, manarmansour2011@yahoo.com f,
had_elghamry@mans.edu.eg g, mohamedelbanna93@gmail.com h, omarhamdy@mans.edu.eg i,*
Received: 12 May 2025 | Revised: 15 June 2025 | Accepted: 28 June 2025 | Published: 04 July 2025
Background: Acinic cell carcinoma (ACC) is an uncommon salivary gland neoplasm that is characterized by its slow growth rate and good survival. The presence of locally aggressive ACC is not a common occurrence.
Case Presentation: A 62-year-old male patient with a medical history of left parotid swelling that underwent a superficial parotidectomy and lymph node dissection one year earlier elsewhere. The postoperative pathology revealed acinic cell carcinoma and negative lymph nodes (LNs). Two months later, the patient exhibited a left external auditory canal swelling. The swelling was excised elsewhere, and the postoperative pathology revealed ceruminous glands adenocarcinoma. Subsequent to a period of four months, a substantial fungating mass manifested on the entire left side of the face and neck. The patient received three cycles of chemotherapy, yet no satisfactory response was observed. The patient underwent a palliative resection of the fungating parotid lesion. The procedure included a wide local excision (WLE), which entailed the removal of the lesion and surrounding tissue, as well as the excision of the left external ear and facial nerve branches. Additionally, a left lateral block neck dissection was performed, followed by reconstruction using a supraclavicular artery island flap. Postoperative pathology revealed a diagnosis of acinic cell carcinoma, with infiltration of one out of three dissected lymph nodes in the main specimen by tumor tissue. Furthermore, there was infiltration of the surrounding fibrofatty tissue and muscle fibers by tumor tissue. However, the sent 17 cervical lymph nodes were found to be free from tumor deposits. Postoperatively, the patient exhibited optimal wound healing, with no flap loss, and a satisfactory cosmetic outcome when compared to the preoperative status. The patient received postoperative concurrent chemoradiotherapy, then developed lung metastasis five months after surgery. For this subsequent metastasis, the patient received chemotherapy followed by sorafenib. Notwithstanding, the patient’s condition ultimately deteriorated, necessitating referral for best supportive care. The patient died one year after the surgery.
Conclusion: ACC is a rare salivary gland tumor that typically requires surgical resection. Inappropriate management can result in severe disfigurement. In such cases, supraclavicular artery island flap (SCAIF) can serve as a viable reconstructive option..
Keywords: Acinic Cell Carcinoma; Radical Parotidectomy; Treatment Individualization; Supraclavicular Artery Island Flap.
ACC, a rare malignant neoplasm of the salivary glands, predominantly affects white individuals between the ages of fifty and sixty (Cavaliere et al., 2020; Dąbrowski et al., 2011). The onset of the condition is characterized by the gradual development of a solitary, soft, painless, and well-defined mass within the gland over an extended period (Cavaliere et al., 2020; Goldman et al., 2007; Graves et al., 2024). It is challenging to differentiate ACC from benign parotid gland tumors through routine imaging without confirming the diagnosis through tissue biopsy (Cavaliere et al., 2020; Suh et al., 2005). Batsakis classified ACC into two groups, low-grade and high-grade, depending on specific features such as vascular involvement, finger-like tissue invasion, and histological patterns (Gomez et al., 2009; Kirschnick et al., 2021). Given the rarity of the disease, the existing corpus of knowledge on its clinical features and treatment outcomes has been primarily derived from case reports and series. However, these sources have not provided sufficient evidence on the effectiveness of chemotherapy and radiation therapy (Gomez et al., 2009).
In this report, we present a case of a gigantic fungating recurrent ACC of the parotid gland in a 62-year-old male patient. The patient underwent a wide local excision of the tumor, which included the removal of the ear lobule, and subsequent reconstruction of the large defect using a supraclavicular artery island flap (SCAIF).
A 62-year-old male patient with a medical history of left parotid swelling that underwent a superficial parotidectomy and lymph node dissection at an external medical facility. The postoperative pathology revealed acinic cell carcinoma, and seven dissected lymph nodes were found to be negative for malignancy. Two months later, the patient exhibited left external auditory canal swelling, which was excised elsewhere. Postoperative pathology revealed ceruminous gland adenocarcinoma. Four months later, a substantial fungating mass was observed, encompassing the entire left side of the face and neck. Additionally, there was palpable swelling in the upper deep cervical lymph nodes (Figure 1a).
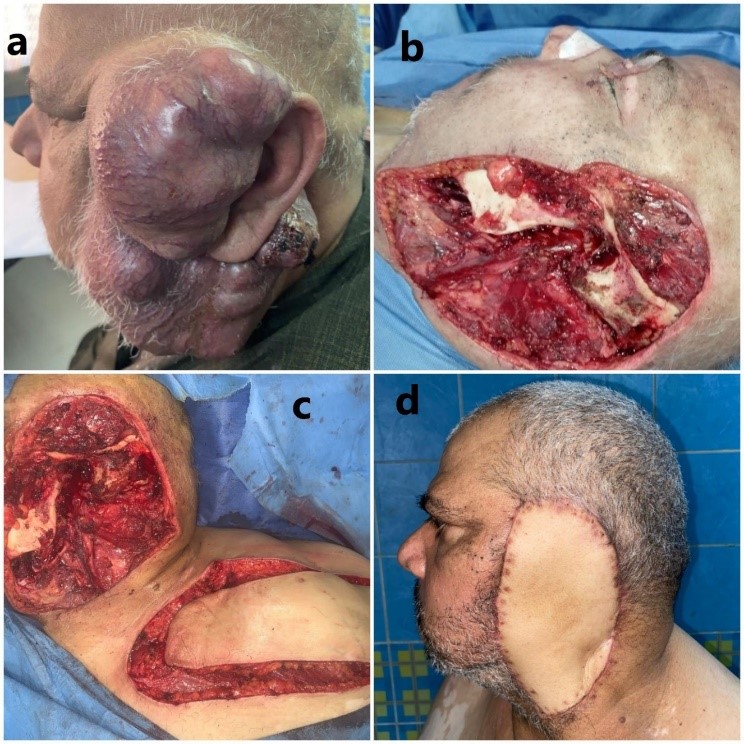
Figure 1. Preoperative, Operative & Post-Operative Photos:
(a) The mass at presentation.
(b) Intraoperative photo after tumor resection.
(c) Intraoperative photo after flap preparation.
(d) Two weeks postoperative
A post-contrast magnetic resonance imaging (MRI) of the head and neck revealed an ill-defined soft tissue swelling at the operative bed of the left parotid gland and preauricular regions. This swelling replaced parenchyma of the parotid gland deep lobe and extended to the left temporomandibular joint. On the lower level, the masses were seen contacting non-separable from the left masseter muscle, left sternomastoid muscle, left submandibular gland, and internal jugular vein with no clear fat planes in between. It has been observed that the structure in question encases both the left superficial temporal artery and the left external auditory canal. The patient exhibited multiple enlarged bilateral levels I and II lymph nodes, with the largest measuring 1 x 1.5 cm and exhibiting a preserved shape and hilum. PET/CT imaging revealed a left parotid operative bed soft tissue mass, as well as enlarged left submandibular, upper, and lower deep cervical lymph nodes measuring 7 x 5 x 12 cm with SUV max 6.7.
The patient received three cycles of chemotherapy (Platinol-Taxol), the last one on August 16, 2021, and no radiotherapy was received. A magnetic resonance imaging (MRI) scan performed in August 2021 revealed the presence of a sizable mass in the left parotid space, characterized by a prominent exophytic component (Figure 2). The dimensions of the mass were recorded as 8.5 x 7.3 x 16 centimeters. Its extension was noted to span superiorly to the suprazygomatic temporal fossa and left parietal region, inferiorly to the level of C4 vertebra, and anteriorly into the left masticator space. The mass appeared to infiltrate the masseter muscle, encasing the left mandibular ramus and potentially causing cortical erosions. The structure was observed to be completely encasing the retromandibular vein in the posterior region, and it appeared to infiltrate the left auricle and the external auditory canal. Furthermore, it was observed to be encasing and widening the stylomastoid foramen, and it was non-separable from the sternomastoid muscle with possible infiltration, it extended superomedially into the medial aspect of the masticator space (infiltrating the pterygoid muscles) and the deep parapharyngeal space. Also, it was seen invading/ compressing the left Eustachian tube with subsequent mastoiditis, infero-medially, extending into deep pharyngeal space, displacing the carotid sheath with no vascular encasement. It was observed adherent to the posterior aspect of the left submandibular gland, with possible infiltration. Multiple discrete malignant enlarged levels Ia, IIb, and V lymph nodes were detected, with the largest measuring approximately 13 x 14 mm.
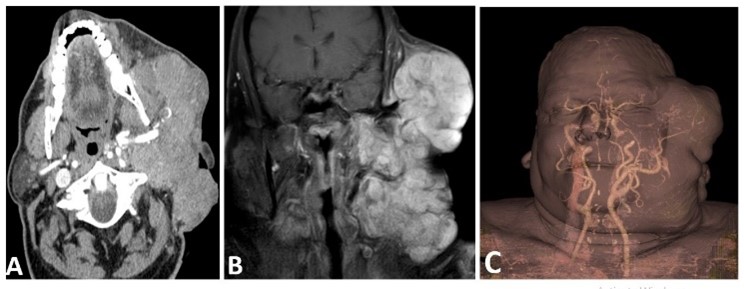
Figure 2. Post-Contrast CT and MR Examination of the Patient
(A) A large lobulated heterogeneously enhancing soft tissue mass is seen in the left parotid space totally encasing the terminal part of the left external carotid artery.
(B) Coronal Post-contrast MR, shows the multi-spacial extension of the mass with suprazygomatic and temporal components superiorly and cervical space inferiorly.
(C) 3D CT angiography of the mass shows the arterial supply from the superficial temporal artery.
The patient underwent Palliative Resection: A wide local excision (WLE) of the fungating parotid lesion was performed, encompassing the left external ear and facial nerve branches. These structures were meticulously removed en-block with the mass. The procedure further involved a left lateral neck dissection and reconstruction utilizing a supraclavicular artery island flap, as depicted in Figure 1.
Postoperative pathology (Figure 3) revealed a diagnosis of acinic cell carcinoma, with infiltration of one out of three dissected lymph nodes in the main specimen by tumor tissue. Furthermore, there was infiltration of the surrounding fibrofatty tissue and muscle fibers by tumor tissue. However, the sent 17 cervical lymph nodes were found to be free from tumor deposits.
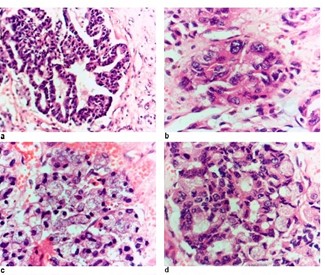
Figure 3. Microscopic examination of the tumor:
(a) Glandular cells showing eosinophilic cytoplasm and vesicular nuclei. The cells are arranged in solid sheets and acinar pattern (X200).
(b) Intercalated duct-like cells that are cuboidal & polygonal showing abundant eosinophilic cytoplasm and centrally-placed pleomorphic nuclei. The cells are arranged in solid sheets (HX&Ex400).
(c) Solid sheet of acinar cells large polygonal cells with abundant basophilic granular cytoplasm and eccentric small hyperchromatic nuclei. (HX&Ex400)
(d) Mixture of non-specific glandular cells and basophilic cells. The cells are arranged in acinar & solid sheet patterns. (HX&Ex400).
Postoperatively, the patient exhibited optimal wound healing, with no flap loss, and a satisfactory cosmetic outcome when compared to the preoperative status. The patient received postoperative concurrent chemoradiotherapy, which consisted of 25 sessions of radiotherapy with Platinol sensitizer administered weekly. The flap demonstrated robust tolerance to the radiotherapy treatment. The patient subsequently exhibited lung metastasis five months following surgical intervention. He was administered chemotherapy (Taxotere followed by Adria carboplatin) and subsequently treated with sorafenib. Notwithstanding, the patient’s condition ultimately deteriorated, necessitating referral for comprehensive supportive care till he died. This referral was issued with the expectation of a duration of care extending up to one year following the initial surgical intervention.
Parotid gland ACC is a slow-growing neoplasm that accounts for between 10% and 18% of malignant tumors and between 2% and 4% of parotid gland neoplasms. The condition predominantly afflicts individuals between the ages of fifty and sixty who identify as white. This phenomenon has been documented in both bilateral cases and pediatric populations (Goldman et al., 2007). The incidence of such advanced parotid gland acinic cell carcinoma is reported to be low in the literature. Presently, the prevention of uncontrolled tumor growth is facilitated by the expeditious implementation of surgical interventions. Moreover, the low incidence and slow growth of these tumors (Goldman et al., 2007) precludes them from growing to the extent previously described. This aspect of the patient’s presentation, disease progression, and management is unique and contributes to the complexity of the case.
Tumor biopsies, preferably those performed with a fine needle, are the preferred method for making a diagnosis, which is often challenging to differentiate from benign lesions (Park et al., 2021). The presented patient’s diagnosis was delayed due to an unplanned prior surgical procedure, and the final diagnosis was reached through a revision of the previous pathology at our center.
Gross examination of the ACC typically reveals a yellow-grey, solid mass (Drut & Giménez, 2008). The gland’s microscopic appearance can vary considerably depending on the cells’ arrangement in different architectural patterns. The presence of solid, papillary, cystic, and follicular cells is a possibility. Typically, positive results from periodic acid–Schiff staining are observed. The biological behavior of a tumor cannot be predicted by the degree of differentiation (Greig et al., 2008). In this case, despite the initial diagnosis of a potentially low-grade tumor, the mass exhibited infiltration of the mandibular region, the masseter muscle, and the area surrounding the auricle.
The prevailing treatment strategy entails a total parotidectomy accompanied by a block neck dissection (Greig et al., 2008; van Weert et al., 2022). A prevailing discourse exists surrounding the potential for omitting the elective block neck dissection in circumstances where radiological evidence of lymph node metastasis is absent, a scenario that is already uncommon in such cases (Laskawi et al., 1998; Moon et al., 2021). In the case presented, the decision to remove the lymph nodes was made in view of the aggressive behavior of the tumor and its infiltration of adjacent structures.
The tumor’s ulceration and aggressiveness resulted in a substantial skin defect following parotidectomy. To address this sequela, a supraclavicular artery island flap (SCAIF) was employed for reconstruction. SCAIF is one of the recently developed surgical techniques in the field of head and neck oncologic reconstruction. The procedure is distinguished by its simplicity, ease of harvest, adequate blood supply, and flexibility. In comparison to pectoralis major flaps, it exhibits a reduced learning curve and operative time. The utilization of this approach has been demonstrated to be associated with a reduced incidence of complications at both the donor and recipient sites, particularly in cases involving fasciocutaneous reconstruction as opposed to mucosal reconstruction (Kokot et al., 2022; Nasr et al., 2023; Poleri et al., 2024; Ru et al., 2024; Sheng et al., 2021). The SCAIF technique was employed as a reconstructive modality in the present patient, yielding optimal color match, comprehensive coverage of the defects, and an absence of postoperative complications.
Acinic cell tumors are a rare form of salivary gland neoplasms that can exhibit unexpected levels of aggression. In the event that such tumors are not managed appropriately, or if they are neglected, severe disfigurement may result. This represents a significant surgical challenge. A comprehensive approach, encompassing meticulous planning, interdisciplinary deliberations, and patient education, is instrumental in ensuring success. A tunneled supraclavicular artery island flap is a viable reconstructive option for addressing tissue defects that result from radical surgical resection.
Ethics approval and consent to participate: All the procedures involving human subjects adhered to the IRB’s ethical requirements, as well as the 1964 Helsinki Declaration and its subsequent revisions. The patient signed a written consent form for the surgical interventions.
Consent for Publication: Available on request
Availability of Data and Material: Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Conflicts of Interest / Competing Interests: The authors declare no conflicts of interest.
Funding: The authors declare that this research received no external funding.
Author Contributions: AE, ME: data collection, and editing SA: supervision, conceptualization & revision. OH: editing, writing & revision. DK, MAG, MM: writing and presentation of the imaging, FE: writing and presentation of the pathology part, HE: revision and editing the clinical oncology part. All authors have read and agreed to the published version of the manuscript.
Acknowledgment: N/A
Cite: Awny, S., M Eid, A., Khedr, D., El-Husseiny, F., Gad, M., Mansour, M., G Elghamery, H., A Elbanna, M., & Hamdy, O. (2025). Surgical Excision of Huge Recurrent Parotid Carcinoma and Reconstruction Using Supraclavicular Artery Island Flap: A Case Report. Middle Eastern Cancer and Oncology Journal, 1(3), 1–5. https://doi.org/10.61706/MECOJ160140
Copyright: © 2025 by the authors. Licensee Scientific Steps International Publishing Services, Dubai, UAE.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


An independent academic publisher with an editorial team including many of the top researchers in the world. SSG publishes research, review, and case report articles in double-blind, peer-reviewed, open access scientific and academic journals.
Copyright © 2025 Scientific Steps International Publishing Services LLC (Dubai – United Arab Emirates)