Volume 1, Issue 1, pp: 1-5
![]()
Diffuse Variant of Nodular Lymphocyte-Predominant Hodgkin Lymphoma
in A 39-Year-Old Female: A Rare Case Report from Syria
Rita Mohammad 1,2*, Haneen Layka2, Salam Bashour3, Sawsan Ismail2,4
1Department of Internal Medicine, Tishreen University Hospital, Lattakia, Syria.
2Cancer Research Centre, Tishreen University Hospital, Lattakia, Syria.
3Department of Internal Medicine, Wahrendorff Hospital, Sehnde, Germany.
4Department of Pathology, Tishreen University, Lattakia, Syria.
E-mail: ritamohammad290@gmail.com1,2*, haneenlayka.97@hotmail.com2, bashoursalam@gmail.com3, sawsanismail8@gmail.com2,4
* Correspondence Author
Received: 17 July 2023 | Revised: 10 November 2023 | Accepted: 11 December 2023 | Published: 15 December 2023
Introduction: Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) represents a rare subtype of Hodgkin Lymphoma that constitutes approximately 5% of all HL cases, with an annual incidence of 1-2 per 1,000,000. Histological diagnosis requires detecting the lymphocyte-predominant (LP) cells, characterized by their popcorn-like contours and distinct immunophenotypic features, including the expression of the B cell surface marker CD20, with negative expression of CD15 and CD30, within a characteristic tumoral microenvironment.
Case Presentation: A 39-year-old Syrian female was admitted to our hospital due to a painless, palpable mass in the left axilla, accompanied by no other symptoms. Three months earlier, the patient noticed the mass and visited an external clinic, where she received a ten-day course of antibiotics without experiencing any improvement. Physical examination revealed a firm, round mass devoid of signs of inflammation. An ultrasonography was performed and identified six enlarged lymph nodes in the left axilla displaying signs indicative of malignancy. These nodes were surgically excised, and the subsequent microscopic examination unveiled a biphasic nodular and diffuse proliferation of small lymphocytes, follicular dendritic cells, and epithelioid histiocytes, mixed with large distinct tumor cells recognized as LP cells, that are characterized by multilobulated nuclei with finely granular chromatin and prominent nucleoli. Immunohistochemical examination demonstrated positive expression for CD20 and CD45 in the LP cells, along with CD57 in the background cells, with negative expression for CD15, CD30, and BCL6, while CD10, CD3, BCL2, and Cyclin D1 markers yielded inconclusive results. Consequently, the final diagnosis was confirmed as NLPHL-Diffuse variant.
Conclusion: In our manuscript, we presented a diagnostically challenging case of NLPHL diffuse variant in a middle-aged otherwise healthy woman. This case emphasizes on the importance of thorough microscopic examination with the use of immunostaining to make an accurate histopathological diagnosis and thus to provide the best possible medical care in similar cases.
Keywords: Classical Hodgkin’s lymphoma; Nodular lymphocyte-predominant Hodgkin lymphoma; Immunohistochemistry; Lymphocyte predominant cells; Lymphocyte-rich T cell\histiocyte- rich large B-cell lymphoma.
Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL) is a rare subtype of Hodgkin Lymphoma that constitutes approximately 5% of all HL cases, with an annual incidence of 1-2 per 1000000 (Eichenauer & Engert, 2017). The first case of NLPHL was described by Rosenthal in 1936 (Rosenthal, 1936), followed by further reports in 1944 by Jackson and Parker, termed lymphocyte-rich paragranuloma (Jackson & Parker, 1944; Moiseeva T.N et al., 2015).
However, NLPHL wasn’t officially recognized as a separate entity from CHL until 2001 in the revised WHO classification of lymphoid malignancies (Lee & LaCasce, 2009; Swerdlow, 2008).
Typically affecting young adults and children, NLPHL displays a male predominance and often exhibits an indolent clinical behavior. Histological diagnosis involves identifying the lymphocyte-predominant (LP) cells, characterized by their popcorn-like contours with distinct immunophenotypic features, including the expression of B cell surface marker (CD20) with negative expression of CD15 and/or CD30 (Lee & LaCasce, 2009; Regula et al., 1988). The diffuse variant is an exceptionally rare histological subtype that necessitates detailed diagnosis. Herein, we present a rare case of the diffuse variant of NLPHL.
A 39-year-old Syrian female was admitted to our hospital due to a painless, palpable mass in the left axilla, accompanied by no other symptoms. Three months ago, the patient noticed the mass and visited an external clinic, where she received a ten-day course of antibiotics without experiencing any improvement. Her surgical and family history were unremarkable, and all laboratory findings were within normal limits, except for a mild elevation of ESR (35mm/h).
During examination, a firm round non-inflammatory mass was palpated, and subsequent ultrasonography revealed enlargement in more than six lymph nodes in the left axilla, measuring between 1.5-2.8 cm in diameter. These masses appeared round with hypoechoic centers and displayed peripheral and hilar vascularity, suggestive of malignancy. Ultrasonography of both right and left breast along with the right axillary lymph nodes showed normal results, while a computed-tomography (CT) scan revealed no other lesions. Following this, the patient underwent surgical excision of the left axillary lymph nodes, revealing a mass measuring 8.5×6×4 cm, consisting of matted encapsulated nodes (10 nodes) with a nodular grey cut surface.
Microscopic examination revealed a biphasic nodular and diffuse proliferation comprising small lymphocytes, follicular dendritic cells, and epithelioid histiocytes interspersed with large, distinct tumor cells known as LP cells. These LP cells are characterized by multilobulated nuclei exhibiting finely granular chromatin and prominent nucleoli (Figure1). The differential diagnosis encompassed nodular lymphocyte predominant Hodgkin lymphoma (NLPHL), follicular lymphoma (FL), and nodal marginal zone lymphoma (NMZL).
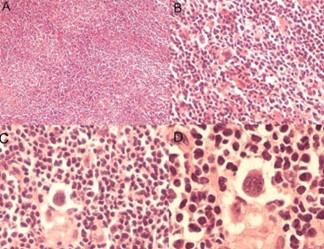
Figure 1. Microscopic Examination of Histopathological Slide of the Axillary Lymph Node Biopsy:
(A) Ill-defined series of nodules and diffuse polymorphous infiltrate [hematoxylin and eosin (H&E) ×40], (B) Lymphocytes admixed with atypical larger forms, few eosinophils, plasma cells, and histiocytes [H&E ×100], (C) Multinucleated giant LP cell [H&E ×200], (D) LP cell at higher magnification [H&E x400].
Immunohistochemical examination demonstrated positive expression of CD20 and CD45 in tumor cells, alongside positive expression of CD57 in the background T cells. Conversely, it demonstrated negative expression of CD15, CD30, and BCL6, while results of CD10, CD3, BCL2, and Cyclin D1 were inconclusive. As a result, the final diagnosis was confirmed as NLPHL-Diffuse variant (Figure 2).
The patient underwent a whole-body multi-slice contrast-enhanced computed tomography (CT) scan, which did not reveal any other significant abnormalities. Subsequently, a positron-emission tomography (PET) scan was performed for initial staging. The PET scan indicated hypermetabolic soft tissue edema in the left axilla, a result consistent with recent surgical intervention (excisional biopsy). Additionally, bilateral cervical lymphadenopathy was revealed, with the largest node on the right measuring 10×17mm with an increased 18F-FDG marginal uptake, with a maximum standardized uptake value (SUV) of 2.8 which was not considered as a malignancy. No evidence of distant metastasis was found. According to the ANN-ARBOR system for HL, we diagnosed her as stage IA NLPHL. The patient received no treatment apart from the complete resection of the left axillary mass and monitored regularly with PET scans at periodic intervals for 2 years to detect any potential relapses. The most recent PET scan detected no signs of malignant lesions.
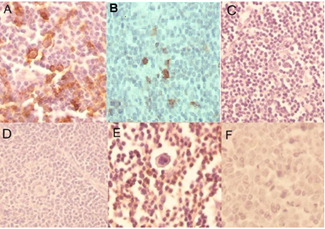
Figure 2. Histopathological slide of Immunohistochemistry Stains of the Axillary Lymph Node Biopsy:
(A) Positive cytoplasmic expression of CD20 (IHC x200), (B) Positive T cells of CD57 (IHC x100), (C) Negative expression of CD15 (IHC x100), (D) Negative expression of CD30 (IHC x100), (E) Negative expression of CD3 (IHC x200), (F) Negative expression of Bcl-6 (IHC x200).
The diffuse variant of NLPHL is an exceedingly rare variant, accounting for less than 25% of NLPHL cases, as described by Fan et al. The vast majority of cases typically affect young adults and children, showing a male predominance and an indolent clinical behaviour (Fan et al., 2003; Lee & LaCasce, 2009). In our case, the patient was a 39-year-old female. Contrary to the usual presentation of the diffuse variant at an advanced stage (Fan et al., 2003), our patient presented solely with an isolated swelling in the left axillary nodes, alongside a mildly elevated ESR, without any other abnormal results.
Ultrasonography is the primary radiologic method for evaluating axillary lymphadenopathy (Fujioka et al., 2021). In our patient, it revealed 6 enlarged lymph nodes within the left axilla, indicating signs of malignancy. Additionally, the ultrasound image allowed us to exclude metastatic breast cancer, which is primary differential diagnosis in cases of axillary lymphadenopathy.
The current guidelines recommend whole-body contrast-enhanced computerized tomography (CT) scan for assess the extent of malignancy (McKay et al., 2016). In our patient, a CT scan of the neck, chest, abdomen and pelvis revealed no abnormal findings.
Moreover, 18-F fluoro-deoxy-glucose-positron emission computerized tomography (FDG-PET/CT) is considered the gold standard technique for staging according to the ANN-ARBOR staging system (Lister et al., 1989). Accordingly, our patient underwent an FDG-PET/CT scan, which detected a small amount of metabolic activity in the left cervical lymph nodes, registering an SUV of 2.8, deemed benign with no further lesions indicated. Subsequently, the disease was classified as stage IA NLPHL.
Nevertheless, histological and immunohistochemical examinations remain the most reliable procedures to confirm the diagnosis of NLPHL. Typical histologic findings involve the effacement of the lymph node structure by a diffuse and mildly nodular proliferation of lymphocytes, histiocytes, dendritic reticulum cells, and the neoplastic LP cells. The latter are characterized by a popcorn-like nuclear contour, basophilic cytoplasm, and lobulated nuclei, as demonstrated in our case (Lee & LaCasce, 2009).
Immunohistochemical examination is crucial for confirming the diagnosis, characterized by the expression of CD20 along with CD45 and BCL6, while showing negativity for CD15 and CD30. Additionally, T cells, which form rosettes around LP cells, typically positive for CD57 and CD3 (Anagnostopoulos et al., 2000; Younes et al., 2021).
In our case, LP cells displayed positivity for CD45 and CD20 and negativity for CD15 and CD30. Scattered CD57-positive T cells were observed in the background surrounding LP cells. This immunostaining panel supports the diagnosis of a diffuse variant of NLPHL. Other immune stains, such as CD10, BCL-2, and BCL-6 yielded inconclusive results.
The main differential diagnosis includes the lymphocyte-rich subtype of CHL (LR-CHL), distinguished by small B-lymphocyte nodules within a rich inflammatory background.
However, unlike NLPHL nodules, LR-CHL nodules typically exhibit small germinal centers at their edges, a characteristic not observed in NLPHL. Additionally, CD30 and CD15 are expressed in approximately all cases of CHL, which contrasts with NLPHL.
T-cell/histiocyte-rich large B-cell lymphoma (THR-LBCL) presents a significant challenge as another differential diagnosis. Both diagnoses share similar histological and immunophenotypic characteristics, with a few malignant B cells dispersed within a reactive background of histiocytes and lymphocytes. Moreover, the neoplastic cells of THR-LBCL might exhibit popcorn-like nuclear contours resembling those observed in LP cells of NLPHL.
However, according to the latest edition of the Who classification, THR-LBCL is defined by a complete loss of nodular architecture and the absence of follicular dendritic cell (FDC) meshworks. Therefore, a detailed microscopic examination and the detection of even one nodule suffice to exclude the diagnosis of THR-LBCL (Anagnostopoulos et al., 2000; Hartmann & Eichenauer, 2020).
The treatment approach for NLPHL depends on the disease stage. According to the latest version of NCCN guidelines, involved-site radiation therapy (ISRT) is recommended for asymptomatic patients in early disease stages. This recommendation emphasizes that most deaths are related to secondary malignancies and chemotherapy-related toxicities rather than the disease itself (NCCN, 2021). However, this treatment approach is typically restricted to stage IA patients with a solitary lymph node involvement completely removed by biopsy which aligns with our patient’s case. Yet, the presence of histopathological variants may alter the treatment strategy.
Some studies advise against a ‘watch and wait’ strategy for patients with diffuse histological variants (Bessen et al., 2021). However, a recent study of two cases showed that these variants have not significantly influenced treatment decisions (Spinner et al., 2019).
This was the case of our patient who underwent treatment solely through complete excision of the affected lymph nodes despite the presence of the histological diffuse variant. The patient chose a ‘’watch and wait’’ approach due to planning for pregnancy, she was monitored regularly with PET scans at periodic intervals of 6 months. The most recent PET scan indicated complete remission of the disease.
In our manuscript, we report a diagnostically challenging case of the diffuse variant of NLPHL in a middle-aged, healthy woman. This case illustrates the extreme difficulty in diagnosing this rare subcategory of HL, marked by its distinctive immunohistochemical expression and characteristic tumoral microenvironment. Addressing these diagnostic complexities is crucial to offer the best possible medical care for such cases.
Cite: Mohammad, R., Layka, H., Bashour, S., & Ismail, S. (2023). Diffuse Variant of Nodular Lymphocyte-Predominant Hodgkin Lymphoma in A 39-Year-Old Female: A Rare Case Report from Syria. Steps Journal for Pathology and Laboratory Medicine, 1(1), 1–5. https://doi.org/10.61706/sjplm14001

Copyright: © 2023 by the authors. Licensee SSG, Dubai, UAE.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND 4.0) license (http://creativecommons.org/licenses/by-nc-nd/4.0/).


An independent academic publisher with an editorial team including many of the top researchers in the world. SSG publishes research, review, and case report articles in double-blind, peer-reviewed, open access scientific and academic journals.
Copyright © 2025 Scientific Steps International Publishing Services LLC (Dubai – United Arab Emirates)