ISSN: 3080-1427 (online) / 3080-1419 (print)
Volume 1, Issue 3 (July 2025 – September 2025), pp: 10-17
![]()
Patterns of Use of the Oncotype DX Breast Recurrence Score® Test
in a Kurdish Population of Patients with Breast Cancer:
A Multi-Institutional, Retrospective Study
Hawro T. Hamza 1,a, Fahmi M. Salih 2,b, Sami S. Omar 2,3,4,c,*,
Kalthuma S. Hamadamin 5,d, Tara A. Abdulrazzaq 1,e, Kakil I. Rasul 6,f
1 Department of Oncology, Nanakali Hospital, Azadi street, Erbil, Kurdistan, Iraq.
2 Rizgary Oncology Center, Peshawa Qazi Street, Erbil, Kurdistan, Iraq.
3 Faculty of Medicine, Koya University, Koya, Erbil, Iraq.
4 Kscien Organization, Hamid Str, Azadi Mall, Sulaimani, Iraq.
5 Department of Pathology, Rizgary Teaching Hospital, Peshawa Qazi Street, Erbil, Kurdistan, Iraq.
6 National Cancer Care and Research, Hamad Medical Corporation, Doha 3050, Qatar.
E-mail: hawrotaha@gmail.com a, fzebary@yahoo.com b, sami.saleem@live.com c,*,
kalthumalab2020@gmail.com d, dr.tararoyal@gmail.com e, kakil1954@gmail.com f
Received: 23 May 2025 | Revised: 14 July 2025 | Accepted: 12 August 2025 | Published: 06 September 2025
Oncotype DX (ODX) is widely used to predict recurrence risk and guide treatment in early-stage, estrogen receptor-positive, HER2-negative breast cancer by analysing 21 genes to provide a recurrence score (RS). Validated in clinical trials, it is endorsed by major organizations like NCCN, ASCO, and ESMO. In the Kurdistan Region of Iraq, ODX is funded by the Cancer Patients’ Support Fund (CPSF), but access remains inconsistent. This study aimed to investigate the patterns of Oncotype DX Breast Recurrence Score® test utilization in a Kurdish population of patients with breast cancer, highlighting challenges and opportunities for optimizing patient selection and clinical benefit while addressing financial considerations. This retrospective study in the Kurdistan region of Iraq (2018-2023) involved 300 patients with luminal-type early-stage breast cancer. Data on demographics, tumor characteristics, and Oncotype DX Recurrence Scores® were analyzed to assess test usage patterns. Descriptive statistics were applied, and ethical approval was obtained from all participating centers. The median age of patients was 52 years (range 26-87), with 98.3% being female. Mastectomies were performed in 36% of cases, while 59% had breast-conserving surgeries. Axillary node-positive disease was present in 2.4%, with a median of 6 lymph nodes resected. Most patients had unifocal (76.3%) disease, and invasive ductal carcinoma was the dominant histology (83%). Tumors were primarily grade II (62.9%), with lymphovascular invasion in 17.1% and perineural invasion in 16.1%. Recurrence scores (ORS) were low, intermediate, and high in 16.7%, 54.5%, and 23.4% of cases, respectively. This study provides key insights into breast cancer patients in the Kurdistan region, particularly regarding the use of the Oncotype DX Breast Recurrence Score® test. Most patients were female, with left-sided and invasive ductal carcinoma being more prevalent. The study highlights gaps in sentinel lymph node biopsy implementation and delays in test turnaround times due to healthcare infrastructure challenges.
Keywords: Oncotype DX, Breast Cancer, Recurrence Score, Genomic Testing, Kurdistan Region.
In clinical practice, there has been an increasing use of gene expression profiling tests to predict the probability of recurrence and personalize treatment for individuals diagnosed with early-stage breast cancer (BC) (Reis-Filho & Pusztai, 2011).
Among the available tests is Oncotype DX (ODX) Breast Recurrence Score®, a validated genomic test developed by Exact Sciences in Madison, Wisconsin, USA. This test calculates a recurrence score (RS) for patients diagnosed with early-stage, estrogen-receptor (ER)-positive breast cancer. The diagnosis of HER2-negative invasive breast cancer is made on the basis of the expression of 21 genes—16 cancer-related genes and 5 reference genes—in formalin-fixed paraffin-embedded (FFPE) tumor tissue samples. This diagnosis is made using reverse transcription polymerase chain reaction (RT-PCR) (Kim et al.). The following text is intended to provide a comprehensive overview of the subject matter. 2011). The assay has been demonstrated to display the prognosis of patients with early-breast cancer, and to inform on the chemotherapy benefit added to endocrine therapy (Albain et al., 2010; Paik et al., 2006) and the risk of distant recurrence with endocrine therapy alone (Sparano et al., 2018). It also provides a single recurrence score (RS), ranging from 0 to 100 (Paik et al., 2004).
Prospective, phase 3 randomized clinical trials involving thousands of patients have confirmed its validity. Patients are initially classified into three risk groups based on the Recurrence Score (RS): low (RS 0-18), intermediate (18-30), and high (31-100). Subsequent refinement of this classification resulted in the identification of two distinct categories: low (0-25) and high (RS 26-100). This refinement was informed by the patient’s age, with categories delineated based on whether the patient was above or below the age of 50. The findings of the research demonstrate that a low RS value is associated with a considerably lower risk of distant recurrence and a reduced likelihood of benefiting from chemotherapy. Conversely, a high RS value indicates a higher risk of distant recurrence and predicts a significant benefit from chemotherapy (Albain et al., 2010; Dowsett et al., 2010; Kalinsky et al., 2021a, 2021b; Paik et al., 2004, 2006; Sparano et al., 2018).
The incorporation of RS into treatment decision-making has been integrated into numerous clinical guidelines, including those issued by the National Comprehensive Cancer Network (NCCN) (Breast Cancer, 2024), the American Society of Clinical Oncology (ASCO) (Andre et al., 2022), and the European Society of Medical Oncology (ESMO) (Loibl et al., In the year 2024, the St Gallen International Expert Consensus guidelines (Burstein et al., 2021) and the UK National Institute for Health and Care Excellence (NICE) Guidelines (1 Recommendations | Tumour Profiling Tests to Guide Adjuvant Chemotherapy Decisions in Early Breast Cancer | Guidance | NICE, n.d.) were consulted. In this paper, we present an account of our experience with the utilization of genomic tools in the context of treatment decision-making for early-stage breast cancer in Kurdistan, Iraq. Our analysis aims to elucidate prevalent patterns and address the challenges encountered, while concurrently identifying areas that present opportunities for further exploration. The objective of this study is to determine the most suitable patients for the Oncotype DX test. This will ensure that the test provides the greatest possible clinical benefit while minimizing financial burden.
The present research adopted a retrospective observational design, conducted over a period of five years (2018–2023). The objective of the study was to evaluate the utilization patterns of the Oncotype DX Breast Recurrence Score® (ODX) test in patients with luminal-type, early-stage breast cancer in the Kurdistan Region of Iraq.
The study was conducted in four major oncology centers across the Kurdistan Region: The following medical facilities have been identified as oncology centers: Rizgary Oncology Center, Nanakali Hospital, Hiwa Hospital, and Azadi Oncology Center. A comprehensive understanding of ODX test usage was provided by the analysis of data retrieved from institutional records.
Patients were included if they met the following conditions:
Patients were excluded from the study if they:
The test is available free of charge to any eligible patient. However, this is not always the case. This phenomenon is not exclusive to our region; significant disparities in the utilization of ODX among oncologists, patient populations, and geographical areas have been observed in other developed countries as well. These disparities are supported by compelling evidence (Matikas et al., 2019; Zhu et al., 2021). The selection of patients was contingent upon the availability of complete medical records, including histopathology reports and immunohistochemistry results. The evaluation of ER, PR, and HER2 status was conducted in accordance with ASCO/CAP guidelines (Allison et al., 2020; Wolff et al., 2023). Furthermore, Ki-67 expression levels were evaluated by local pathologists employing a standardized and reliable method (Penault-Llorca & Radosevic-Robin, 2017).
Patient demographic information, tumor characteristics (size, grade, hormone receptor status, histology), and ODX Recurrence Score® results were extracted from electronic medical records. The assessment of Ki-67 expression levels was conducted by local pathologists, employing standardized methodologies to ensure the consistency and reliability of the results.
The study protocol received ethical clearance from the institutional review boards of all participating oncology centers. In accordance with the principles of confidentiality and ethical standards, all patient data were anonymized.
Descriptive statistics were performed using SPSS software to summarize patient demographics, tumor characteristics, and Recurrence Score® results. Furthermore, time intervals associated with the testing process, including the period from surgery to test request and result, were analyzed to ascertain potential delays and their ramifications.
A total of 299 patients were included in the study. The median age of the patients was 52 years (range 26-87 years). The majority of the patients were female, with 98.3% (n = 295) of the subjects being female and 1.7% (n = 5) of the subjects being male (Table 1). The surgical approaches employed in the study cohort are outlined as follows: 21.4% (n = 64) of patients underwent Modified Radical Mastectomy (MRM) with Axillary Lymph Node Dissection (ALND), while 7% (n = 21) had MRM with Axillary Lymph Node Sampling (ALNS), and 7.4% (n = 22) underwent MRM with Sentinel Lymph Node Biopsy (SLNB). Among the patients who underwent breast-conserving surgery, 14.4% (n = 43) underwent Wide Local Excision (WLE) with ALND, 11.4% (n = 34) underwent WLE with ALNS, and 31.8% (n = 95) underwent WLE with SLNB. A mere 1.3% of the sample (n = 4) exhibited WLE without the concomitant axillary procedure. However, data concerning the surgical approach was missing or unknown in 5.4% of cases (n = 16) (Table 2). The median number of resected lymph nodes among the entire cohort was six lymph nodes (range: 0-41) (Table 2). Furthermore, only 2.4% of patients exhibited axillary node-positive disease (Table 3). A comparative analysis revealed that left-sided breast cancers exhibited a slightly higher prevalence (47.5%) compared to right-sided breast cancers, with only 2.3% of the cases manifesting bilateral breast tumors. The patient population exhibited a prevalence of unifocal or multifocal disease, with 76.3% (n=228) affected by unifocal disease and 18.7% (n=56) by multifocal disease. The predominant histological classification was identified as invasive ductal carcinoma, accounting for 83% of cases, in contrast to the 13% prevalence of invasive lobular carcinoma. The majority of the tumors were classified as grade II (62.9%), with lymphovascular invasion and perineural invasion documented in 17.1% (n=51) and 16.1% (n=48), respectively (Table 3). The Ki-67 proliferation index was evaluated in the study population. The results indicated that 43% of patients exhibited a Ki-67 index of ≤14%, while 45.5% of patients demonstrated a Ki-67 index of >14%. Furthermore, Ki-67 data was missing or unknown in 11.4% of the cases.
The Oncotype Dx Recurrence Score results were as follows: low, 16.7%; intermediate, 54.5%; and high, 23.4% (Table 4).
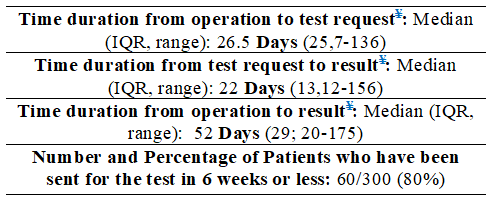
As illustrated in Table 5, the following data is presented: time intervals associated with the Oncotype DX Breast Recurrence Score® test process for patients who underwent surgery. The temporal framework is delineated as such: Time Duration from Operation to Test Request: The median time interval from the surgical operation to the request for the Oncotype DX test was 26.5 days, with an interquartile range (IQR) and range spanning from 25 to 136 days. This interval signifies the duration required for oncologists to evaluate the necessity for the test and initiate the request. The second row of data presents the duration of the process, measured from the submission of the test request to the release of the result. The median interval from the test request date to the result release date was 22 days, with an interquartile range (IQR) of 13 to 156 days. This interval is indicative of the turnaround time for the Oncotype DX test, a critical component in decision-making regarding adjuvant therapy. The third row of data corresponds to the duration of the operation, from the initialization to the attainment of the desired result. The median overall time interval from the date of surgery to the receipt of the Oncotype DX test result was 52 days, with an interquartile range (IQR) and range of 29 to 175 days. This combined duration is of critical importance as it reflects the entire process, from surgery through to the availability of test results for guiding postoperative treatment. As indicated by the final row in Table 5, a significant proportion of patients were referred for testing within a brief timeframe following their surgical procedures. Specifically, the data reveals that 80% of patients underwent testing within a period of less than one week subsequent to their surgical operations.
Table 1. Patient Demographics
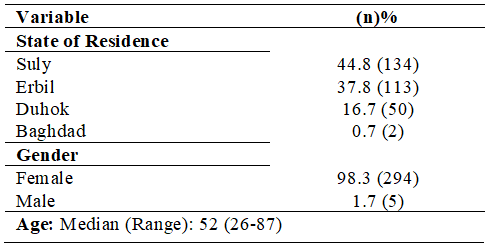
Table 2. Distribution of Surgical Approaches and Resected Lymph Node Count in Patients with Early-Stage Breast Cancer
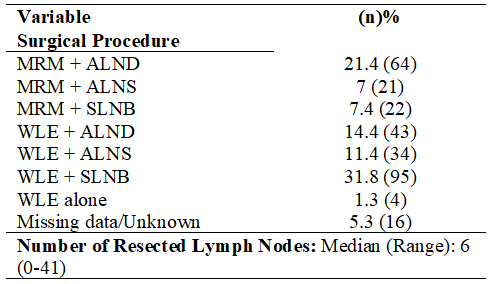
Table 3. Tumor and Immunohistochemical Characteristics
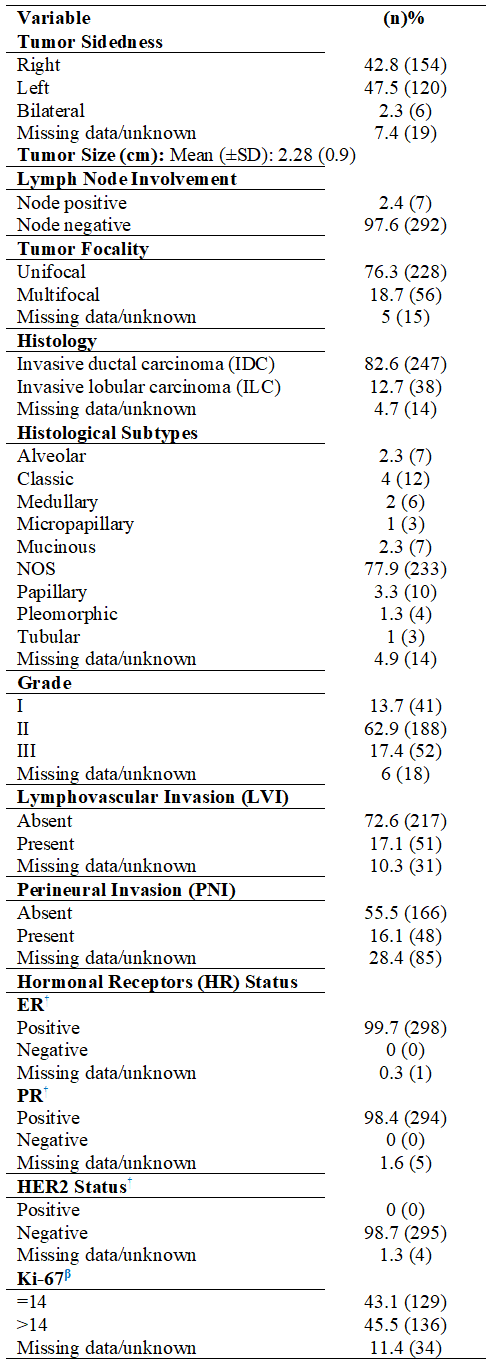
Table 4. Stratification of Early Breast Cancer Patients by Nottingham Prognostic Index and Oncotype DX Categorical Scores
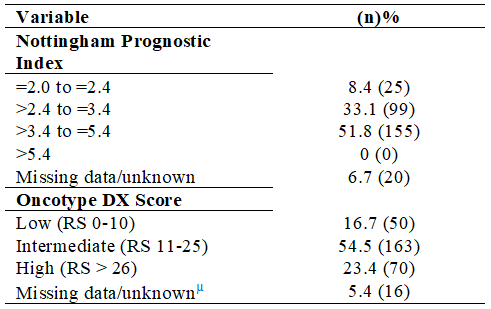
Table 5. Time Durations from Surgery to Test Request and Test Result
This study offers pivotal insights into the clinicopathological characteristics and utilization patterns of the Oncotype DX Breast Recurrence Score® (ODX) within a Kurdish patient cohort. The demographic is predominantly female (98.3%) and has a median age of 52 years, aligning with global trends observed in pivotal trials such as TAILORx.
This consistency in patient profiles selected for genomic testing internationally is underscored (Sparano et al., 2018).
The observation that left-sided breast cancers exhibited a slightly higher prevalence (47.5%) compared to right-sided breast cancers aligns with the findings of international epidemiological studies, suggesting a potential link between anatomical or genetic predispositions and a higher incidence of left-sided breast cancer (Abdou et al., 2022; Perkins et al., 2004). The clinical relevance of this laterality may involve differential lymphatic drainage or variations in hormonal receptor distribution, possibly influencing recurrence risk and therapeutic outcomes, thus warranting further investigation (Amer, 2014).
Sentinel lymph node biopsy (SLNB) remains underutilized in the Kurdistan region, reflecting broader infrastructural and educational challenges within surgical oncology. The lower adoption rate (38 cases with SLNB vs. 162 cases with ALND) underscores substantial training and resource disparities, which have the potential to adversely impact patient morbidity and quality of life through unnecessary axillary dissections, elevated complication rates, and diminished functional outcomes (Giuliano et al., 2017; Krag et al., 2010). The American Society of Clinical Oncology (ASCO) guidelines explicitly recommend SLNB as the standard of care for early-stage breast cancer, underscoring its importance in reducing complications while maintaining oncologic safety (Lyman et al., 2017).
The predominant histological manifestation of invasive ductal carcinoma (82.6%) is consistent with global data, which consistently identifies this subtype as the most prevalent (Ciriello et al., 2015; Desmedt et al., 2016). The most prevalent type of tumor was Grade II, accounting for 62.9% of cases. This finding indicates an intermediate level of aggressiveness and biological complexity. It underscores the critical importance of precise genomic profiling in guiding adjuvant treatment decisions. Tumor grade has been shown to have a significant correlation with prognosis and treatment responsiveness, underscoring the importance of a comprehensive histopathological evaluation combined with genomic assessments (Rakha et al., 2010).
Lymphovascular invasion (LVI) and perineural invasion (PNI), identified in 17.1% and 16.1% of cases, respectively, have been shown to be clinically significant markers of aggressive tumor behavior and poorer prognosis. The presence of these features necessitates careful consideration of more aggressive adjuvant treatment strategies, as they indicate increased metastatic potential. This underscores the utility of genomic assays in precisely stratifying risk (Zhang et al., 2023).
The distribution of Oncotype DX Recurrence Scores revealed a majority (54.5%) in the intermediate-risk category (RS 11-25). This categorization poses a clinical challenge, as decision-making in intermediate-risk patients frequently necessitates careful patient-physician discussions about treatment preferences and the balance of chemotherapy risks versus benefits, especially in the absence of clear-cut clinical guidelines (Andre et al., 2022; Cheng et al., 2018; Sparano et al., 2018).
The turnaround time for obtaining ODX results, which averaged 52 days from operation to result, is significantly longer than the ideal standards recommended for initiation of adjuvant therapy. Generally, adjuvant therapy should commence within 4 to 6 weeks post-surgery for optimal clinical outcomes (Ashok Kumar et al., 2019; Gagliato et al., 2014). Such delays may compromise therapeutic effectiveness by potentially allowing microscopic metastatic dissemination, thus adversely impacting survival outcomes. The mitigation of these delays may be achieved through the streamlining of logistical pathways and the enhancement of local laboratory capabilities or regional partnerships. These measures have the potential to improve timely therapeutic interventions and patient prognoses.
This study underscores significant infrastructural and educational gaps in genomic testing and surgical practices within the region. It highlights the critical need for policy reforms, resource allocation, and training enhancements to fully leverage the benefits of precision oncology. Further research is needed to elucidate the biological implications of tumor laterality and to refine risk stratification models, particularly within intermediate-risk patient populations. This will foster more individualized and effective breast cancer treatment strategies.
This study offers significant insights into the clinicopathological characteristics of breast cancer patients in the Kurdistan region of Iraq and the patterns of use of the Oncotype DX Breast Recurrence Score® test in this population. The median age of patients was 52 years, with the majority being female and left-sided breast cancer being slightly more prevalent. The study under scrutiny emphasizes the predominance of invasive ductal carcinoma and the significant proportion of patients with intermediate Oncotype DX Recurrence Scores. Despite the advances in breast cancer management, this study highlights deficiencies in the implementation of sentinel lymph node biopsy and delays in test result turnaround times, primarily attributable to regional healthcare infrastructure challenges.
In addition, further exploration is necessary to elucidate the correlation between tumor biology and Recurrence Scores, as well as the side of breast cancer. This investigation is particularly salient in light of international reports indicating poorer outcomes for left-sided breast cancers. These findings contribute to the ongoing discourse on optimizing breast cancer management, emphasizing the need for improvements in surgical expertise, access to diagnostic tests, and the timely delivery of genomic testing results. This study underscores the importance of applying personalized treatment approaches based on genomic assays like the Oncotype DX test. It also highlights areas for improvement in breast cancer care in the region. Future research and policy changes should aim to address these gaps to enhance patient outcomes.
Ethics approval and consent to participate: The study protocol received ethical clearance from the institutional review boards of all participating oncology centers. In accordance with the principles of confidentiality and ethical standards, all patient data were anonymized.
Consent for Publication: Not applicable.
Availability of Data and Material: The data that supports the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest / Competing Interests: The authors declare that there are no conflicts of interest.
Funding: The authors declare that this research received no external funding.
Author Contributions: H.T.H: Software, Writing – original draft, reviewing and editing. F.M.S: Methodology, Software and Data curation. S.S.O: Data curation, writing of the original draft and project administration. K.S.H, T.A.A: Validation, Investigation and writing and reviewing and editing. K.I.R: Conceptualization, Visualization and project administration.
Acknowledgment: Not applicable
Use of Generative AI and AI-Assisted Technologies: The authors declare that no generative AI or AI-assisted technologies were used in the preparation of this work.
Cite: Hamza, H. T., Salih, F. M., Omar, S. S., Hamadamin, K. S., Abdulrazzaq, T. A., & Rasul, K. I. (2025). Patterns of Use of the Oncotype DX Breast Recurrence Score® Test in a Kurdish Population of Patients with Breast Cancer: A Multi-Institutional, Retrospective Study. Middle Eastern Cancer and Oncology Journal, 1(3), 10-17. https://doi.org/10.61706/MECOJ160157
Copyright: © 2025 by the authors. Licensee Scientific Steps International Publishing Services, Dubai, UAE.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


An independent academic publisher with an editorial team including many of the top researchers in the world. SSG publishes research, review, and case report articles in double-blind, peer-reviewed, open access scientific and academic journals.
Copyright © 2025 Scientific Steps International Publishing Services LLC (Dubai – United Arab Emirates)