ISSN: 3080-1427 (online) / 3080-1419 (print)
Volume 1, Issue 2 (April 2025 – June 2025), pp: 13-18
![]()
Multiple Hepatic Epithelioid Hemangioendothelioma; A Rare Case Report
Basak Barzngy 1,a* , Sawen Dizay 2,b, Sami S. Omar 1,3,4,c, Tamara A. Almufty 5,d, Fairuz A. Kakasur 2,e, Savan Saeed 6,f
1 Rizgary Oncology Center, Peshawa Qazi Street, Erbil, Kurdistan, Iraq.
2 Rizgary Teaching Hospital, Peshawa Qazi Street, Erbil, Kurdistan, Iraq.
3 Kscien Organization, Hamid Str, Azadi Mall, Sulaimani, Iraq.
4 Faculty of Medicine, Koya University, Koya, Iraq.
5 Maternity Teaching Hospital, Shorish street, erbil, Iraq.
6 Hawler Medical University, College of Medicine, Khanzad Street, Erbil, Iraq.
E-mail:
barzngybasak@gmail.com a,*, sawendizay81@gmail.com b, sami.saleem@live.com c , tamaramufty@yahoo.com d, doctorsh7@gmail.com e, Savan.shengola@hmu.edu.krd f
Received: 31 January 2025 | Revised: 28 March 2025 | Accepted: 25 April 2025 | Published: 12 May 2025
Introduction: Epithelioid hemangioendothelioma (EHE) is a very rare vascular tumor. It is characteristically locally aggressive and can arise from soft tissue and bone. There is diagnostic confusion between EHE and other benign and malignant vascular tumors. A WWTR1-CAMTA1 translocation fusion gene is found in 90% of conventional EHE.
Case Report : A 44-year-old woman was found to have two hepatic lesions after evaluation for right-sided hypochondrial pain. Biopsy of the largest lesion was found to be EHE. Immunohistochemistry showed positivity of tumor cells for CD31 & CD34. A staging CT scan and PET scan were performed and both ruled out other lesions elsewhere in the body. A right hepatectomy was performed. Three lesions were found. All were EHE. The first nodule was found near the portal vein and measured 3×2.6x2cm. The second and third nodules were 1.5×1.5cm and 8mm respectively. After surgery, the patient is under regular follow-up and monitoring. She is still free from any recurrence.
Discussion : Multiple hepatic epithelioid hemangioendothelioma (EHE) is a diagnostic challenge when there is still a lack of appropriate active and reproducible treatment options for it. Studies show that most EHE present with multiple liver masses. The definitive diagnosis of EHE is based on histopathology ranging from paucicellular to moderately cellular lesions. On FDG-PET scans, EHE typically show moderate FDG activity. The diagnosis of our case was challenging due to the presence of an occult mass that was not detectable on any imaging modality. Both liver transplantation and liver resection have been discussed; the latter strategy was used in our case.
Conclusion: EHE is a very rare vascular tumor that arises from the cells lining the blood vessels. EHE is a locally aggressive tumor. Hepatic EHE usually presents as multiple masses in the liver. It has its own immunohistochemical and genetic characteristics. Surgery is the mainstay of treatment.
Keywords: Epithelioid Hemangioendothelioma, Multiple Liver Masses, Vascular Tumor.
Epithelioid vascular tumors comprise a diverse group of benign to highly malignant tumors with a broad histologic spectrum including epithelioid hemangioma, epithelioid hemangioendothelioma (EHE), and epithelioid angiosarcoma (O’Connell et al., 2001; Sheng et al., 2013; Wenger & Wold, 2000). EHE is a rare, locally aggressive vascular tumor that can arise in soft tissue, bone, and visceral organs (Requena & Kutzner, 2013). Cases of EHE arising from the heart with involvement of surrounding vessels have also been reported (Huang et al., 2021). The incidence of EHE is less than one person per 1,000,000 person-years. Although some studies suggest that EHE is more common in women (Lau et al., 2011; Stacchiotti et al., 2021), other studies don’t support this (Liu & He, 2022). Because this tumor has an epithelioid morphology, it often causes diagnostic confusion with other epithelioid vascular neoplasms as well as carcinomas (Nakagawa et al., 1986). While a WWTR1-CAMTA1 fusion gene is found in 90% of conventional EHE (Errani et al., 2011; Requena & Kutzner, 2013), a histologically distinct subset of EHE has been shown to harbor a separate fusion gene, YAP1 TFE3 (Antonescu et al., 2013). Immunohistochemically, EHE is positive for CD31 and CD34 (may be negative) while negative for S100, SOX10, Desmin, EMA and SMA (Flucke et al., 2014; Mentzel et al., 1997).
Hepatic EHE, on CT scan, appears as low attenuation nodules especially in the hepatic subcapsular region. Initially, the hepatic lesions appear as solitary nodules, later the nodules may coalesce to form confluent masses (Epelboym et al, 2019). In addition, peripheral enhancement and a halo pattern have been seen on post-contrast images (Kehagias et al., 2000; Lin & Ji, 2010; Lyburn et al., 2003). On MRI, liver lesions are hypointense on T1-weighted images and hyperintense on T2-weighted images (Amin et al., 2011; Epelboym et al., 2019). EHE has an aggressive clinical course with a tendency for regional lymph node metastasis, nearby organ invasion, and local recurrence (Lau et al., 2011). Here, we present a rare case of multiple liver EHE. Currently, there are no standardized guidelines for the treatment of hepatic EHE. Treatment options are diverse with variable outcomes and include chemotherapy, ablation, surgery, and liver transplantation (Frezza et al., 2021; Virarkar et al., 2020). Compared to other malignant liver tumors, hepatic EHEs have a relatively favorable prognosis. One study found that 50% of patients survived more than five years without treatment, and the presence of metastases did not affect survival (Kou et al., 2020).
A 44-year-old woman presented with right-sided hypochondrial pain of one month’s duration in October 2020. An abdominal ultrasound and CT scan revealed two hypovascular, highly suspicious, enhancing solid lesions in the right lobe of the liver (Figure 1). The masses were centrally necrotic with peripheral cellular enhancement. The lesions were radiologically inconsistent with hemangioma or adenoma. The largest mass was 2 cm while the other was 1 cm in size. Tissue biopsy was taken from the largest one, the result showed cores of liver tissue with steatosis involved by a dense fibrotic lesion containing spindle cells and round plasmacytoid cells with mild pleomorphism. The nuclei were vesicular with small inconspicuous nucleoli. A few mitotic figures were seen. The features were those of a low-grade malignant lesion (Figure 2). The differentials were wide including primary liver lesions such as epithelioid hemangioendothelioma, metastatic carcinoma, and epithelioid sarcoma. Immunostaining showed positivity of tumor cells for CD31 & CD34 while it was associated with negativity for Fli-1, Dog-1 & CD117. Heppar & AE1/3 were negative in the lesion and positive in the background normal liver. The features were those of a vascular lesion and consistent with epithelioid hemangioendothelioma. Because of further concern, a staging PET scan was performed and showed the following findings; the liver measured 18.8 cm in the craniocaudal direction. A hypodense FDG-avid lesion with an SUVmax of up to 5.76 and a size of 2.3 x 2.9 x 3.0 cm was noted in segment VIII of the liver (Figure 3). Based on the above findings, curative surgery with right hepatectomy was decided. Right hepatectomy was performed and the biopsy was done in a different center from the pathology department where the core biopsy was examined. Gross findings showed that the liver measured 19x15x10cm, and the attached gallbladder measured 9.5×4.5cm. Three nodules were found on sectioning. The first nodule was located near the portal vein and measured 3×2.6x2cm. The second nodule was near the gallbladder and measured 1.5×1.5cm. The third nodule measured 8 mm. Microscopic examination of all three nodules showed infiltration by high-grade malignant cells with large pleomorphic nuclei, prominent nucleoli with abundant cytoplasm, arranged in single cells, cords, and strands with occasional glandular formation associated with extensive desmoplastic stroma. The remainder of the liver showed mild to moderate macrovesicular steatosis. The gallbladder was unremarkable. Based on the above findings, a new immunohistochemistry was performed on the resected masses. The new IHC showed strong and diffuse positivity of the tumor cells for CD31, which was tested on two separate masses. CK7, anti-hepatocyte antibody and AE1/3 stained the trapped biliary canaliculi and hepatocytes but were negative in the malignant cells. Glypican 3 was negative within the tumor area (Figure 4). The overall features were consistent with multiple epithelioid hemangioendothelioma of the liver. Since then, the patient has been under regular follow-up and surveillance, and she is still doing well with no recurrence.
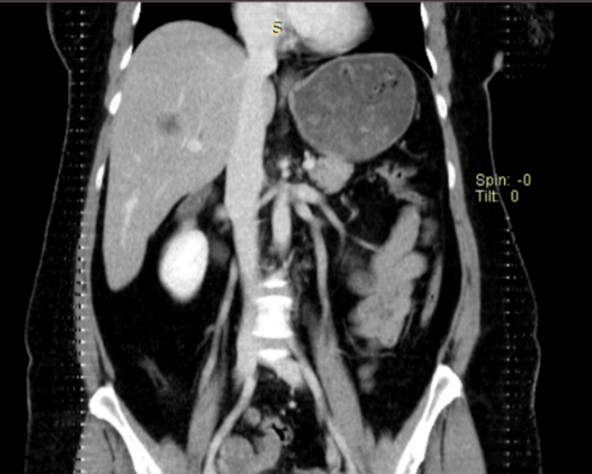

Figure 1. CT Scan Showing Hypovascular Lesion.
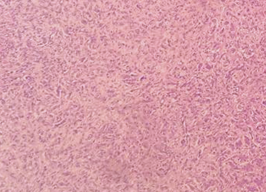
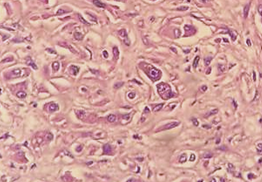
Figure 2. (A) Low Power View Showed Multiple cords of Cells with an Infiltrative Growth Pattern Set in a Dense Fibrohyalin Stroma. (B) High Power View, Showed Endothelial Cells with Large Nucleus, Prominent Nucleoli, Abundant Cytoplasm with Occasional Intracellular ‘Capillary’ Luminal Space.
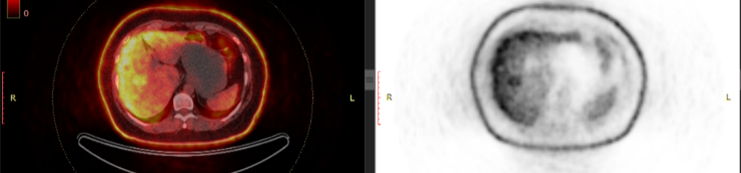
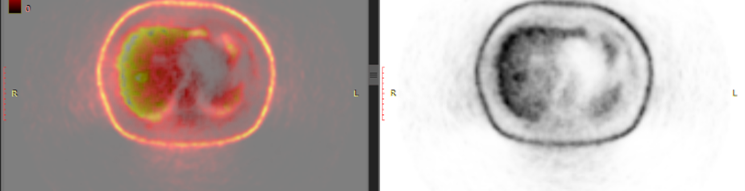
Figure 3. FDG PET Scan Showing an FDG Uptake Lesion in Segment 8.
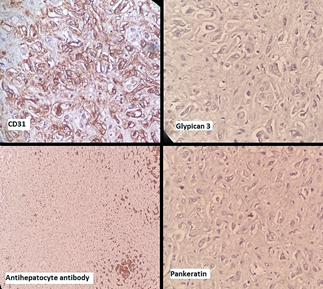
Figure 4. Immunohistochemical Staining Showed Strong Positivity for CD31 While Negative for Glypican 3, Antihepatocytes Antibody and Pankeratin.
Epithelioid hemangioendothelioma (EHE) is an ultra-rare vascular endothelial neoplasm with characteristic histology and discrete fusion genes (e.g., WWTR1-CAMTA1 gene fusion) (Kallen & Hornick, 2021). The presence of the WWTR1-CAMTA1 fusion is a hallmark genetic alteration in most cases of EHE and serves as a specific biomarker for diagnosis. It helps to differentiate EHE from other vascular neoplasms with overlapping histopathologic features. Fluorescence in situ hybridization (FISH) and next-generation sequencing (NGS) are commonly used to detect this fusion. The correct diagnosis of EHE is still a clinical challenge, and we still lack appropriate active and reproducible treatment options for EHE. Most patients present with non-specific clinical complaints related to right hypochondrial pain (Jurczyk et al., 2014). Our case presented multiple liver lesions mimicking cavernous hemangioma, multifocal hepatocellular carcinoma, peripheral cholangiocarcinoma and metastatic lesions on CT scan. Therefore, the management of such cases with multiple liver masses is very challenging and a thorough evaluation is crucial. The mean age of the patients in a case series study (Makhlouf et al., 1999) was 47 years, which is compatible with the age of our patient, who is 44 years old. The final diagnosis of HEH is based on histopathology. EHEs range from paucicellular to moderately cellular lesions. They are composed of spindle cells and epithelial cells that are either seen as single cells or arranged in clusters (Kamarajah et al., 2018). IHC study showing positive staining for endothelial markers: 94% of tumors are positive for CD34, and 86% of them are positive for CD31 (Dong et al., 2013; Ishak et al., 1984). Our case showed positive staining for both. In a study that included 137 cases of hepatic EHE, 82% of the cases, like our case, had multiple hepatic EHE. In addition, only 14.5% of the cases had unilobar liver lesions, while the others had diffuse liver lesions (Kaltenmeier et al., 2022). On PET/CT, EHE shows variable but usually moderate FDG activity. A retrospective study showed that the SUVmax of the most metabolically active lesion in the liver ranged from 2.6 to 10.5 with a mean of 5.1±2.1 (Frota Lima et al., 2021). The SUVmax of our case was up to 5.76 and had a size of 2.3 x 2.9 x 3.0cm. Due to its heterogeneity and variable clinical outcome, an appropriate treatment strategy for EHE has not yet been developed (Fan et al., 2020). Both liver transplantation and liver resection have been discussed, and the latter strategy was used in our case (Bachmann et al., 2003). A study published in Clinical Cancer Research demonstrated that the TAZ-CAMTA1 fusion protein promotes tumorigenesis by upregulating connective tissue growth factor (CTGF), which in turn activates the Ras-MAPK pathway. This finding led to the initiation of a phase II clinical trial (SARC033) to evaluate the efficacy of trametinib, a MEK inhibitor, in patients with unresectable or metastatic EHE (Ma et al., 2022).
There are difficulties and challenges in the diagnosis of EHE, as it is often confused with other lesions radiologically and histopathologically, and the multiplicity of the tumor makes the diagnosis more challenging. Especially from the histopathologic point of view, it requires a team to decide.
EHE is a very rare vascular tumor that arises from the cells lining the blood vessels. EHE is locally aggressive and its diagnosis is challenging. The presentation of this tumor as multiple masses makes EHE confused with multifocal hepatocellular carcinoma, peripheral cholangiocarcinoma and metastatic lesions. Immunohistochemically they are both CD31 & CD34 positive and genetically the WWTR1-CAMTA1 fusion gene is found in almost all cases. The main treatment strategy for EHE is surgery, either liver resection or transplantation. Postoperative surveillance is still accepted.
Cite: Barzngy, B., Dizay, S., Omar, S. S., Almufty, T. A., Kakasur, F. A., & Saeed, S. (2025). Multiple Hepatic Epithelioid Hemangioendothelioma; A Rare Case Report. Middle Eastern Cancer and Oncology Journal, 1(2), 13–18. https://doi.org/10.61706/MECOJ160131
Copyright: © 2025 by the authors. Licensee Scientific Steps International Publishing Services, Dubai, UAE.
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


An independent academic publisher with an editorial team including many of the top researchers in the world. SSG publishes research, review, and case report articles in double-blind, peer-reviewed, open access scientific and academic journals.
Copyright © 2025 Scientific Steps International Publishing Services LLC (Dubai – United Arab Emirates)