Middle Eastern Cancer and Oncology Journal (MECOJ)
ISSN: 3080-1427 (online) | 3080-1419 (print)
Volume 2, Issue 2 (April 2026 – June 2026) Pages 1-10
Comparative Outcomes of Salvage Therapy in Relapsed and Refractory Hodgkin and Non-Hodgkin Lymphomas in Iraq
1 Medical Oncology Department, AL Jawad Oncology Center, Baghdad, Iraq.
2 The National Center of Hematology, Mustansiriyah University, Baghdad, Iraq.
Abstract
Lymphoma is a relatively treatable cancer, characterized by a favorable prognosis. Nevertheless, between 10% and 25% of patients will exhibit primary refractory or recurrent illness, despite the implementation of risk-adapted treatments. The objective of this study is to assess the response of Hodgkin and non-Hodgkin lymphoma to salvage therapy. A retrospective cohort study was conducted, encompassing 110 patients diagnosed with refractory/relapsed Hodgkin's lymphoma (HL) and non-Hodgkin lymphoma (NHL). The study period spanned from March 2022 to October 2022. Patient demographic and clinical data were meticulously collected for the purpose of analysis. The patients received salvage therapy and were closely monitored to assess their response to the treatment. The results indicate a mean age of 36.07 years ± 14.028 years. Of the patients in the study, 59 (53.6%) were diagnosed with Hodgkin's lymphoma (HL), while 51 (46.4%) were diagnosed with non-Hodgkin's lymphoma (NHL). The most prevalent type of HL was nodular sclerosis, accounting for 38 cases (64.4%). The majority of NHL cases were classified as DLBCL (41 cases, 80.4%). Subsequent to the administration of initial line management, the relapse rate was found to be 48.2%, while the refractory rate was determined to be 51.8%. Following the administration of second-line management, the complete/partial response rate was found to be 73.6%, with a significant association observed between this response rate and Hodgkin's lymphoma (HL). Patients were treated with ABVD as a first-line therapy and ICE as a second-line therapy. In addition, the relapse rate following second-line management was 26.4%, exhibiting a significant association with non-Hodgkin's lymphoma (NHL) with a p-value less than 0.05. For HL, the most effective salvage protocol was identified as ICE, while for NHL, no significant difference was identified among salvage protocols.
Keywords: Salvage Therapy, Relapses, Refractory, Hodgkin Lymphomas, Non-Hodgkin Lymphomas.
Introduction
Lymphomas are a diverse collection of cancers that have the potential to affect any part of the body. These neoplasms frequently originate in the lymph nodes but can metastasize to other anatomical regions. A total of 1,502 Iraqi patients were diagnosed with Hodgkin lymphoma (HL) during the five-year period from 2000 to 2004, while 5,025 Iraqi patients were registered with Non-Hodgkin lymphoma (NHL) during the four-year period from 2015 to 2018, as reported by the Iraqi Ministry of Health (Al-Mosawi, 2022). However, the recent national statistics are limited in scope. Nevertheless, these figures remain the most comprehensive available from the Iraqi Ministry of Health. For this reason, they were used to contextualize disease burden in this setting. Classical Hodgkin lymphoma constitutes almost 95% of all Hodgkin lymphoma cases, is predominantly observed in young adults, and exhibits an excellent overall prognosis with an approximate 80% cure rate (Amraee et al., 2019; Metzger & Mauz‐Körholz, 2019). According to the Cancer Statistics Review, 1975-2015 - SEER Statistics, the projected percentage of males constituting the patient population newly diagnosed with HL in 2017 is approximately 56%. Patients diagnosed with Hodgkin lymphoma frequently manifest B symptoms, which include significant unexplained weight loss, elevated fevers, and excessive night sweats (Gaut & Schiller, 2019).
In instances where patients demonstrated no response to treatment or exhibited disease progression within three months of completing first-line chemotherapy (CT), they were designated as refractory (Refr). Patients were designated as early relapsed (E-Rel) if relapse was diagnosed between three and twelve months after the conclusion of first-line CT, and as late relapsed (L-Rel) if relapsed occurred beyond twelve months (Edgren et al., 2012). A study by Marie José Kersten et al. (2020) found that from 10% to 30% of patients with chronic lymphocytic leukemia (CLL) experience relapse or primary refractory (R/R) after initial treatment.
Neoplasms of the lymphoid tissues, which are more prevalent in the elderly, can develop from several cell types, including B cell precursors, mature B cells, T cell precursors, and mature T cells. A notable example is non-Hodgkin lymphoma (NHL). The categorization of the condition, as determined by its prognosis, falls into two distinct classifications: "indolent" or "aggressive." (Zhang et al., 2008).
One possible method for memorizing this information is by employing the acronym APLES, which stands for the following five risk factors: The inclusion criteria for this study were as follows: (i) patients must be 60 years of age or older, (ii) have an Eastern Cooperative Oncology Group performance status of more than 1, (iii) have more than one extra-nodal site of illness, and (iv) be in stage III or IV (Cuker et al., 2019).
In instances where HL has relapsed or demonstrated resistance to treatment, the primary objective is the management of the disease with salvage chemotherapy. A substantial body of research has demonstrated that the outcomes observed in patients undergoing salvage chemotherapy serve as a reliable predictor of survival outcomes following high-dose chemotherapy and an autologous stem cell transplant. This assertion is supported by numerous studies (Gutierrez-Delgado et al., 2003; Martín et al., 2001; Sureda et al., 2001). Patients with relapsed or refractory Hodgkin and non-Hodgkin lymphomas have found hope in ESHAP, a low-toxicity salvage treatment that combines etoposide, steroids, ara-C, and cisplatin (Aparicio et al., 1999; Martin et al., 2008).
In certain cases of diffuse large B-cell lymphoma (DLBCL) that recur following initial frontline therapy, multiagent combination chemotherapy has been observed to induce responses; however, at conventional dosages, this approach is not widely regarded as curative. The most prevalent salvage treatments encompass R-DHAP (rituximab, dexamethasone, high-dose Ara-C, and cisplatin), R-ICE (rituximab with ifosfamide, carboplatin, and etoposide), or gemcitabine in conjunction with a platinum, most often GDP (gemcitabine, dexamethasone, and cisplatin) (Kaushansky et al., 2021). To the best of our knowledge, this study is the first to systematically evaluate and compare the effectiveness of multiple salvage chemotherapy protocols for both Hodgkin's lymphoma (HL) and non-Hodgkin's lymphoma (NHL) in an Iraqi cohort. It addresses an evidence gap in the region, where treatment decisions are often based on data from Western populations with different demographic and clinical profiles. The objective of this study is to evaluate the response of Hodgkin and non-Hodgkin lymphoma to salvage therapy and to correlate salvage protocols with prognostic factors.
Patients and Methods
A retrospective cohort study was conducted using data stored in the medical records of all transplant-eligible patients referred to the Autologous Blood and Marrow Transplant Program at Baghdad Teaching Hospital with relapsed/refractory Hodgkin's lymphoma (HL) and non-Hodgkin's lymphoma (NHL) between January 2019 and July 2022.
The study population included 110 patients between the ages of 15 and 65 years who had been diagnosed with biopsy-proven Hodgkin's lymphoma (HL) and non-Hodgkin's lymphoma (NHL). The patients had experienced disease recurrence or had been resistant to initial chemotherapy, and they had received subsequent salvage chemotherapy.
Primary refractory HL and NHL were defined as progressive disease during primary chemotherapy or within three months of its completion. The following data were obtained: age, sex, HB, LDH, performance status, extra nodal involvement, B symptoms, and stage.
Ethical approvals were obtained from the Council of the Iraqi Board of Medical Specialization. The data entry and statistical analysis were conducted using two software programs: Microsoft Excel 2016 and SPSS (Statistical Package for the Social Sciences) Version 26. The impact of the independent variable was assessed through the implementation of a chi-square test (or a Fisher's exact test) of association, with the objective of conducting a comparative analysis of proportions and the subsequent examination of the resulting data. To ascertain the statistical significance of the observed differences among the variables, an independent sample t-test was employed. Statistically significant results were defined as those with a P value less than 0.05.
Results
The present study encompassed a total of 110 patients, with a mean age of 36.07 years (±14.028 years). The study population included 59 patients diagnosed with Hodgkin lymphoma (HL), with a mean age of 30.22 years (±10.853), and 51 patients diagnosed with non-Hodgkin lymphoma (NHL), with a mean age of 42.84 years (±14.323). A statistically significant difference was observed between the two groups (P < 0.001).
The most prevalent form of HL in this study was identified as nodular sclerosis, representing 38 cases (64.4%), followed by mixed cellularity HL, which accounted for 20 cases (33.9%). The most prevalent form of non-Hodgkin's lymphoma (NHL) was identified as diffuse large B-cell lymphoma (DLBCL), accounting for 41 cases (80.4%) (Figure 1).
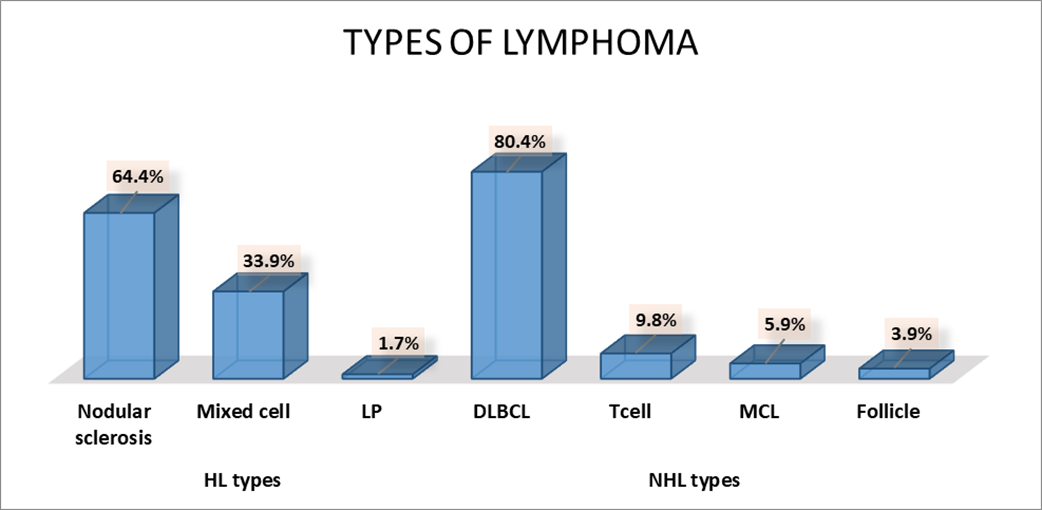
Figures 1. Types of Lymphoma; LP: Lymphocyte-Predominant; Diffuse Large B-Cell Lymphoma: DLBCL; MCL: Mantle Cell Lymphoma.
According to the management, the initial therapeutic modality administered to the patient population was ABVD, which was utilized by 59 patients (53.6%). The RCHOP regimen was employed in the treatment of 51 patients (46.4%). The second line of therapy administered was ice, utilized by 45 (40.9%) patients, followed by RICE, used by 31 (28.2%) patients, GDP, used by 13 (11.8%) patients, RDHAP, used by 9 (8.2%) patients, RGDP, used by 9 (8.2%) patients, and DHAB, used by 3 (2.7%) patients (Figure 2).
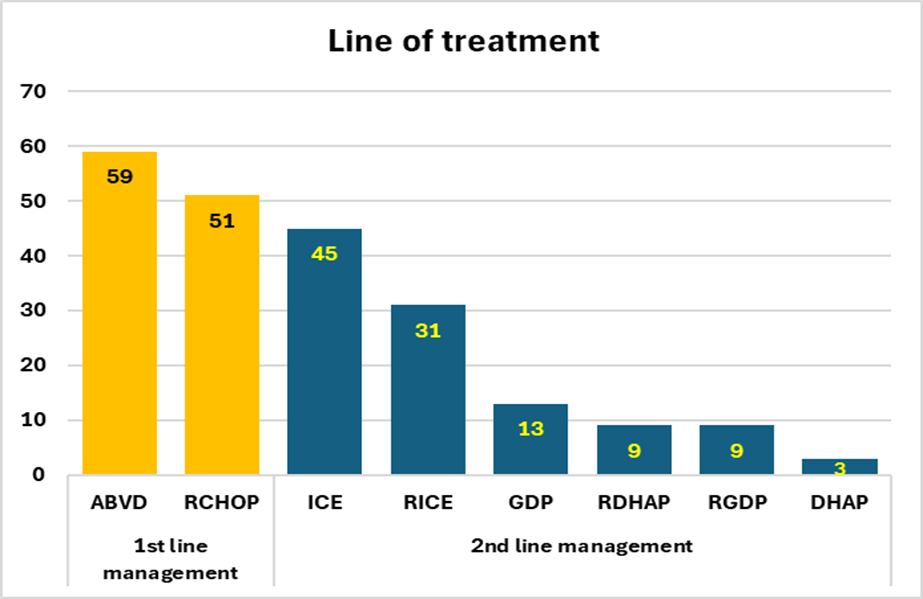
Figure 2. Lines of Management Among Studied Sample
The initial management strategy resulted in a relapse among 53 (48.2%) patients and refractory disease among 57 (51.8%) patients. As illustrated in Figure 3, the results of the second-line management exhibited a complete response in 81 (73.6%) patients and a partial response in 29 (26.4%) patients.
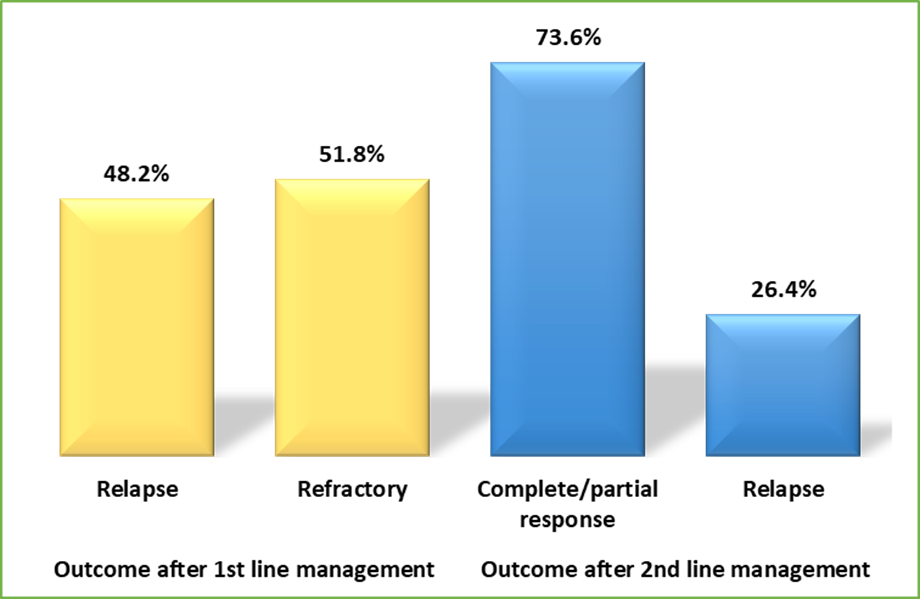
Figure 3. Outcomes Among Studied Sample According to the Lines of Management
The distribution of characteristic features of patients according to diagnosis is elucidated in Table 1. HL was found to be elevated in female subjects and in the initial and secondary stages of the disease (P = 0.004 and P < 0.001, respectively).
The NHL prevalence appeared to be considerably elevated among the elderly population (aged ≥ 60 years) and among patients with a PS of 1 (P < 0.001 and P = 0.002, respectively).
The distribution of outcomes following initial and secondary management of patients according to diagnosis was elucidated in 1. Relapse after second-line management was observed to be significantly higher among patients with non-Hodgkin's lymphoma (NHL), while complete or partial response was observed to be significantly higher among patients with Hodgkin's lymphoma (HL) (P = 0.001).
Table 1. Distribution of Characteristic Features and Outcome of Patients According to the Diagnosis
| Variables | Total | Diagnosis | P* value | ||||
|---|---|---|---|---|---|---|---|
| HL | NHL | ||||||
| No. | % | No. | % | ||||
| Age group/years | < 20 | 13 | 11 | 84.6% | 2 | 15.4% | <0.001 |
| 20 – 39 | 57 | 37 | 64.9% | 20 | 35.1% | ||
| 40 – 59 | 32 | 11 | 34.4% | 21 | 65.6% | ||
| ≥ 60 | 8 | 0 | 0.0% | 8 | 100.0% | ||
| Sex | Male | 61 | 25 | 41.0% | 36 | 59.0% | 0.004 |
| Female | 49 | 34 | 69.4% | 15 | 30.6% | ||
| Hb | Anemic | 59 | 27 | 45.8% | 32 | 54.2% | 0.08 |
| Not anemic | 51 | 32 | 62.7% | 19 | 37.3% | ||
| LDH | High | 43 | 20 | 46.5% | 23 | 53.5% | 0.24 |
| Normal | 67 | 39 | 58.2% | 28 | 41.8% | ||
| Stage | 1st and 2nd | 38 | 30 | 78.9% | 8 | 21.1% | <0.001 |
| 3rd | 34 | 12 | 35.3% | 22 | 64.7% | ||
| 4th | 38 | 17 | 44.7% | 21 | 55.3% | ||
| Ps | 0 | 88 | 54 | 61.4% | 34 | 38.6% | 0.002 |
| 1 | 22 | 5 | 22.7% | 17 | 77.3% | ||
| 2 | 0 | 0 | 0.0% | 0 | 0.0% | ||
| 3 | 0 | 0 | 0.0% | 0 | 0.0% | ||
| Extra nodal | Yes | 31 | 13 | 41.9% | 18 | 58.1% | 0.14 |
| No | 79 | 46 | 58.2% | 33 | 41.8% | ||
| B symptoms | A | 51 | 24 | 47.1% | 27 | 52.9% | 0.25 |
| B | 59 | 35 | 59.3% | 24 | 40.7% | ||
| Outcome after 1st line management | Relapse | 53 | 28 | 52.8% | 25 | 47.2% | 1 |
| Refractory | 57 | 31 | 54.4% | 26 | 45.6% | ||
| Outcome after 2nd line management | Complete/partial response | 81 | 51 | 63.0% | 30 | 37.0% | 0.001 |
| Relapse | 29 | 8 | 27.6% | 21 | 72.4% | ||
| *Chi2 test (or Fisher's Exact test) | |||||||
A complete or partial response to the second line of management was found to be significantly associated with non-anemic patients, normal LDH, the first and second stages of lymphoma, and zero PS without extra nodal involvement, with a p-value of less than 0.05 (Table 2).
Table 2. Distribution of Characteristic Features of Patients According to the Outcome After 2nd Line Management
| Variables | Outcome after 2nd line management | P* value | ||||
|---|---|---|---|---|---|---|
| Complete/partial response | Relapse | |||||
| No. | % | No. | % | |||
| Age group/years | < 20 | 11 | 84.6% | 2 | 15.4% | 0.37 |
| 20 – 39 | 42 | 73.7% | 15 | 26.3% | ||
| 40 – 59 | 24 | 75.0% | 8 | 25.0% | ||
| ≥ 60 | 4 | 50.0% | 4 | 50.0% | ||
| Sex | Male | 41 | 67.2% | 20 | 32.8% | 0.12 |
| Female | 40 | 81.6% | 9 | 18.4% | ||
| Hb | Anemic | 38 | 64.4% | 21 | 35.6% | 0.029 |
| Not anemic | 43 | 84.3% | 8 | 15.7% | ||
| LDH | High | 26 | 60.5% | 17 | 39.5% | 0.015 |
| Normal | 55 | 82.1% | 12 | 17.9% | ||
| Stage | 1st and 2nd stages | 37 | 97.4% | 1 | 2.6% | <0.001 |
| 3rd stage | 21 | 61.8% | 13 | 38.2% | ||
| 4th stage | 23 | 60.5% | 15 | 39.5% | ||
| Ps | 0 | 69 | 78.4% | 19 | 21.6% | 0.03 |
| 1 | 12 | 54.5% | 10 | 45.5% | ||
| 2 | 0 | 0.0% | 0 | 0.0% | ||
| 3 | 0 | 0.0% | 0 | 0.0% | ||
| Extra nodal | Yes | 18 | 58.1% | 13 | 41.9% | 0.03 |
| No | 63 | 79.7% | 16 | 20.3% | ||
| B sympt | A | 40 | 78.4% | 11 | 21.6% | 0.38 |
| B | 41 | 69.5% | 18 | 30.5% | ||
| *Chi2 test (or Fisher's Exact test) | ||||||
As indicated by the results presented in Table 3, there was a statistically significant correlation between the presence of a complete or partial response to second-line management and the administration of ABVD as the initial therapy and ICE as the second-line therapy (P = 0.001 and P = 0.048, respectively).
A statistically significant association was identified between the presence of a complete or partial response to the second-line management and patients diagnosed with HL (P = 0.001; Table 3).
Table 3. Distribution of Characteristic Features of Patients According to the Outcome after 2nd Line Management
| Variables | Outcome after 2nd line management | P* value | ||||
|---|---|---|---|---|---|---|
| Complete/partial response | Relapse | |||||
| No. | % | No. | % | |||
| Diagnosis | HL | 51 | 86.4% | 8 | 13.6% | 0.001 |
| NHL | 30 | 58.8% | 21 | 41.2% | ||
| HL | Nodular sclerosis | 32 | 84.2% | 6 | 15.8% | 0.76 |
| Mixed cell | 18 | 90.0% | 2 | 10.0% | ||
| L rich | 1 | 100.0% | 0 | 0.0% | ||
| NHL | DLBCL | 24 | 58.5% | 17 | 41.5% | 0.53 |
| T cell | 2 | 40.0% | 3 | 60.0% | ||
| Follicle | 2 | 100.0% | 0 | 0.0% | ||
| MCL | 2 | 66.7% | 1 | 33.3% | ||
| B symptom | A | 40 | 78.4% | 11 | 21.6% | 0.38 |
| B | 41 | 69.5% | 18 | 30.5% | ||
| 1st line | ABVD | 51 | 86.4% | 8 | 13.6% | 0.001 |
| RCHOP | 30 | 58.8% | 21 | 41.2% | ||
| Outcome after 1st line management | Relapse | 40 | 75.5% | 13 | 24.5% | 0.82 |
| Refractory | 41 | 71.9% | 16 | 28.1% | ||
| 2nd line | ICE | 40 | 88.9% | 5 | 11.1% | 0.048 |
| RICE | 18 | 58.1% | 13 | 41.9% | ||
| GDP | 10 | 76.9% | 3 | 23.1% | ||
| RDHAP | 6 | 66.7% | 3 | 33.3% | ||
| RGDP | 5 | 55.6% | 4 | 44.4% | ||
| DHAP | 2 | 66.7% | 1 | 33.3% | ||
| *Chi2 test (or Fisher's Exact test) | ||||||
Among patients diagnosed with HL who demonstrated a complete or partial response, the most frequently utilized second-line treatment was ICE, accounting for 88.9% of cases, exhibiting no statistically significant variation, as indicated by a P-value of 0.48, as detailed in Table 4.
The most prevalent drug employed as second-line therapy among patients with non-Hodgkin's lymphoma (NHL) who demonstrated complete or partial response was RDHAP, accounting for 66.7% of cases, with no statistically significant discrepancy noted, as indicated by a P-value of 0.95, as shown in Table 4.
Table 4. Distribution of 2nd Line Management of Patients with HL and NHL According to the Outcome
| 2nd line mx | Outcome after 2nd line management | P* value | |||
|---|---|---|---|---|---|
| Complete/partial response | Relapse | ||||
| No. | % | No. | % | ||
| HL management (no. 59) | |||||
| ICE | 40 | 88.9% | 5 | 11.1% | 0.48 |
| GDP | 9 | 81.8% | 2 | 18.2% | |
| DHAB | 2 | 66.7% | 1 | 33.3% | |
| NHL management (no. 51) | |||||
| RICE | 18 | 58.1% | 13 | 41.9% | 0.96 |
| GDP | 1 | 50.0% | 1 | 50.0% | |
| RDHAP | 6 | 66.7% | 3 | 33.3% | |
| RGDP | 5 | 55.6% | 4 | 44.4% | |
| *Chi2 test (or Fisher's Exact test) | |||||
Discussion
Despite therapeutic improvements, 40% to 60% of patients with non-Hodgkin's lymphoma (NHL) will not achieve complete remission (CR) or will experience a recurrence following conventional first-line therapy (Wood et al., 1993).
The present study found that over half of the patients were male and had HL, which is consistent with the findings of Horwitz et al. (2017). In their research, Horwitz et al. found that 64% of patients were male and that 57% of patients were diagnosed with HL. In this study, the mean age of HL patients was found to be significantly lower than that of non-Hodgkin's lymphoma (NHL) patients, aligning with the findings reported by Shahid et al. (2016). This observation suggests a higher frequency of HL in younger individuals and a higher frequency of NHL in older individuals. The decline in HL incidence among the elderly may be attributed to improved diagnostic techniques and the reclassification of some NHL cases previously labeled as HL (Medeiros & Greiner, 1995).
Nodular sclerosis was identified as the most common Hodgkin's lymphoma (HL) subtype, while diffuse large B-cell lymphoma (DLBCL) was the predominant non-Hodgkin's lymphoma (NHL) subtype, consistent with findings from Batgi et al. (2020). In that study, nodular sclerosis comprised 70% of HL cases, and DLBCL constituted 75% of NHL cases (Batgi et al., 2020).
The results of the second-line management indicated a complete or partial response in approximately three-quarters of the patients, while approximately one-quarter of the patients experienced a relapse. A similar observation was made in a study by Gopal et al. (2010). In this study, 51 individuals diagnosed with relapsed/refractory lymphomas were treated with gemcitabine-carboplatin-based salvage therapy. The overall response rate was 67%.
However, these findings did not align with those reported by Zlotnick et al. (2019), who studied 41 patients receiving gemcitabine-carboplatinum-based salvage therapy for relapse or refractory non-Hodgkin's lymphoma (NHL). Their study revealed an overall response rate of 37%. The discrepancy may be attributed to the inclusion of both HL and NHL patients in our study, while the study by Zlotnick et al. exclusively recruited NHL patients. Additionally, the patients in our sample were younger than the patients in theirs, which may reflect differences in patient age and baseline health status. However, as comorbidity data were not systematically collected, this interpretation should be considered with caution.
With regard to HL, the present study observed a higher incidence among females, which contradicts the findings of Radkiewicz et al. (2023). The latter researchers reported a significantly higher incidence of lymphomas among males across all types. The etiology behind the observed differences in the incidence of lymphoma between males and females remains uncertain. However, it has been proposed that these differences may be attributable to variations in exposure to carcinogens in the environment and/or intrinsic differences, including hormonal and immunological elements, tumor biology, and body size, among women and men (Edgren et al., 2012; Pfreundschuh, 2017).
The present study observed that complete/partial response was associated with non-anemic patients, normal LDH, and zero PS, in the context of the response to the second-line management. This finding aligns with the conclusions of the study by Suzuki et al. (2013), which revealed that individuals exhibiting these specific prognostic factors demonstrated a notably lower overall response rate. The patient exhibited hemoglobin levels that were below the lower limit of the normal range and serum LDH levels that were above the upper limit of the normal range. The correlation between non-anemic status, normal LDH levels, and lower stage with improved outcomes is likely indicative of a reduced tumor burden and enhanced marrow reserve. These factors have been associated with increased chemotherapy tolerance and disease control.
The present study has demonstrated that the initial and secondary stages of lymphoma that are not accompanied by extra-nodal involvement exhibit a notable correlation with the response to second-line management. This finding stands in contrast to the conclusions of a study conducted by Moskowitz et al. (2015), which observed that disease stage does not necessarily predict response to salvage therapy. The discrepancy may be attributable to the fact that the study by Moskowitz et al. incorporated a reduced sample size, a factor that has been demonstrated to exert an influence on the outcomes observed.
A statistically significant association was identified between the presence of a complete or partial response to second-line management and the administration of ABVD as the initial therapy followed by ICE as the subsequent therapy. This finding is at odds with the conclusions of a study conducted by Abalı et al. (2008) in which courses of ICE and DHAP were administered to patients with primary refractory or relapsed HL and NHL. Of the 49 patients, 11 (22.5%) achieved complete remission, while 17 (35%) achieved partial remission, resulting in an overall response rate of 57.5%.
The findings of the present study indicated that complete or partial response to second-line management was significantly associated with HL. This association was further substantiated by the observation that the first and second stages of the disease and PS 0 were significantly associated with HL.
The study's limitations are as follows: it was conducted in a single governorate, which may not be representative of the general population; and it had a small sample size, which may have affected the results.
Conclusion
In the present study, HL demonstrated a high level of dominance among younger patients, females, and those in the early stages of the disease. Furthermore, the analysis revealed that HL was associated with complete and partial responses following second-line management. The NHL demonstrated its superiority among elderly patients, males, and in cases involving late stages and relapses subsequent to second-line management. In the context of nonanemic patients with normal LDH levels, early-stage lymphoma, no extranodal involvement, and the utilization of ABVD as the primary treatment regimen, followed by ICE as a secondary treatment, several factors emerged as crucial determinants of complete or partial response to the second-line management approach. Accordingly, the present study recommended the administration of ABVD as the initial line of therapy and ICE as the secondary line of management. The validation of these findings and the exploration of region-specific treatment algorithms that account for local resource availability and patient characteristics are warranted in future multicenter studies with larger sample sizes.
Declarations
Ethics approval and consent to participate
Ethical approvals were obtained from the Council of the Iraqi Board of Medical Specialization.
Consent for Publication
Not applicable.
Availability of Data and Material
The data that supports the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest / Competing Interests
The authors declare that there are no conflicts of interest.
Funding
The authors declare that this research received no external funding.
Author Contributions
R. H: Conceptualization, Methodology, Formal analysis, Investigation, Writing of the original draft.
A.F.A: Conceptualization, Methodology, Writing of the original draft, Supervision.
Acknowledgment
Not applicable
Use of Generative AI and AI-Assisted Technologies
The authors declare that no generative AI or AI-assisted technologies were used in the preparation of this work.
References
- Abalı, H., Ürün, Y., Öksüzoğlu, B., Budakoğlu, B., Yıldırım, N., Güler, T., Özet, G., & Zengin, N. (2008). Comparison of ICE (Ifosfamide-Carboplatin-Etoposide) Versus DHAP (Cytosine Arabinoside-Cisplatin-Dexamethasone) as Salvage Chemotherapy in Patients with Relapsed or Refractory Lymphoma. Cancer Investigation, 26(4), 401–406. https://doi.org/10.1080/07357900701788098
- Al-Mosawi, A. J. (2022). CANCERS IN IRAQ: HALF CENTURY OVERVIEW. The American Journal of Medical Sciences and Pharmaceutical Research, 4(07), 5–38. https://doi.org/10.37547/TAJMSPR/Volume04Issue07-02
- Amraee, A., Evazi, M. R., Shakeri, M., Roozbeh, N., Ghazanfarpour, M., Ghorbani, M., Ansari, J., & Darvish, L. (2019). Efficacy of nivolumab as checkpoint inhibitor drug on survival rate of patients with relapsed/refractory classical Hodgkin lymphoma: a meta-analysis of prospective clinical study. Clinical and Translational Oncology, 21(8), 1093–1103. https://doi.org/10.1007/s12094-018-02032-4
- Aparicio, J., Segura, A., Garcerá, S., Oltra, A., Santaballa, A., Yuste, A., & Pastor, M. (1999). ESHAP is an active regimen for relapsing Hodgkin's disease. Annals of Oncology, 10(5), 593–595. https://doi.org/10.1023/A:1026454831340
- Batgi, H., Merdin, A., Dal, M. S., Kızıl Çakar, M., Yıldız, J., Başçı, S., Uncu Ulu, B., Yiğenoğlu, T. N., Darçın, T., Şahin, D., Bakırtaş, M., Tetik, A., İskender, D., & Altuntaş, F. (2020). The effect of gemcitabine, dexamethasone, and cisplatin chemotherapy in relapsed/refractory NHL and HL patients: A single center experience. Journal of Oncology Pharmacy Practice, 26(8), 1857–1863. https://doi.org/10.1177/1078155220905654
- Cancer Statistics Review, 1975-2015 - SEER Statistics. (n.d.). Retrieved https://seer.cancer.gov/archive/csr/1975_2015/index.html
- Cuker, Adam., Altman, J. K., Gerds, A. T., & Wun, Ted. (2019). ASH-SAP: American Society of Hematology self-assessment program. American Society of Hematology. https://doi.org/10.1182/ashsap7.chapter23
- Edgren, G., Liang, L., Adami, H.-O., & Chang, E. T. (2012). Enigmatic sex disparities in cancer incidence. European Journal of Epidemiology, 27(3), 187–196. https://doi.org/10.1007/s10654-011-9647-5
- Gaut, D., & Schiller, G. J. (2019). Hematopoietic stem cell transplantation in primary central nervous system lymphoma: a review of the literature. International Journal of Hematology, 109(3), 260–277. https://doi.org/10.1007/s12185-019-02594-1
- Gopal, A. K., Press, O. W., Shustov, A. R., Petersdorf, S. H., Gooley, T. A., Daniels, J. T., Garrison, M. A., Gjerset, G. F., Lonergan, M., Murphy, A. E., Smith, J. C., & Pagel, J. M. (2010). Efficacy and safety of gemcitabine, carboplatin, dexamethasone, and rituximab in patients with relapsed/refractory lymphoma: a prospective multi-center phase II study by the Puget Sound Oncology Consortium. Leukemia & Lymphoma, 51(8), 1523–1529. https://doi.org/10.3109/10428194.2010.491137
- Gutierrez-Delgado, F., Holmberg, L., Hooper, H., Petersdorf, S., Press, O., Maziarz, R., Maloney, D., Chauncey, T., Appelbaum, F., & Bensinger, W. (2003). Autologous stem cell transplantation for Hodgkin's disease: busulfan, melphalan and thiotepa compared to a radiation-based regimen. Bone Marrow Transplantation, 32(3), 279–285. https://doi.org/10.1038/sj.bmt.1704110
- Horwitz, S. M., Hamadani, M., Fanale, M. A., Feingold, J., Spira, A. I., Fields, P. A., Menne, T., Karnad, A., Moskowitz, A. J., Hildyard, C., He, S., Boni, J., & Collins, G. (2017). Interim Results from a Phase 1 Study of ADCT-301 (Camidanlumab Tesirine) Show Promising Activity of a Novel Pyrrolobenzodiazepine-Based Antibody Drug Conjugate in Relapsed/Refractory Hodgkin/Non-Hodgkin Lymphoma. Blood, 130(Supplement 1), 1510–1510. https://doi.org/10.1182/BLOOD.V130.SUPPL_1.1510.1510
- Kaushansky, Kenneth., Lichtman, M. A., Prchal, J. T., Levi, Marcel., Burns, L. J., & Linch, D. C. (2021). Williams hematology (10th ed.). McGraw-Hill.
- Marie José Kersten, Julia Driessen, Josée M. Zijlstra, Wouter J. Plattel, Franck Morschhauser, Pieternella J. Lugtenburg, Pauline Brice, Martin Hutchings, Thomas Gastinne, Roberto Liu, Coreline N. Burggraaff, Marcel Nijland, Sanne H. Tonino, Anne I.J. Arens, Roelf Valkema, Harm van Tinteren, Marta Lopez-Yurda, Arjan Diepstra, Daphne De Jong, & Anton Hagenbeek. (2020). Combining brentuximab vedotin with dexamethasone, high-dose cytarabine and cisplatin as salvage treatment in relapsed or refractory Hodgkin lymphoma: the phase II HOVON/LLPC Transplant BRaVE study. Haematologica, 106(4), 1129–1137. https://doi.org/10.3324/haematol.2019.243238
- Martin, A., Conde, E., Arnan, M., Canales, M. A., Deben, G., Sancho, J. M., Andreu, R., Salar, A., Garcia-Sanchez, P., Vazquez, L., Nistal, S., Requena, M.-J., Donato, E. M., Gonzalez, J. A., Leon, A., Ruiz, C., Grande, C., Gonzalez-Barca, E., & Caballero, M.-D. (2008). R-ESHAP as salvage therapy for patients with relapsed or refractory diffuse large B-cell lymphoma: the influence of prior exposure to rituximab on outcome. A GEL/TAMO study. Haematologica, 93(12), 1829–1836. https://doi.org/10.3324/haematol.13440
- Martín, A., Fernández‐Jiménez, M. C., Caballero, M. D., Canales, M. A., Pérez‐Simón, J. A., García de Bustos, J., Vázquez, L., Hernández‐Navarro, F., & San Miguel, J. F. (2001). Long‐term follow‐up in patients treated with Mini‐BEAM as salvage therapy for relapsed or refractory Hodgkin's disease. British Journal of Haematology, 113(1), 161–171. https://doi.org/10.1046/j.1365-2141.2001.02714.x
- Medeiros, L. J., & Greiner, T. C. (1995). Hodgkin's disease. Cancer, 75(1 Suppl), 357–369. https://doi.org/10.1002/1097-0142(19950101)75:1+<357::aid-cncr2820751318>3.0.co;2-a
- Metzger, M. L., & Mauz‐Körholz, C. (2019). Epidemiology, outcome, targeted agents and immunotherapy in adolescent and young adult non‐Hodgkin and Hodgkin lymphoma. British Journal of Haematology, 185(6), 1142–1157. https://doi.org/10.1111/bjh.15789
- Moskowitz, A. J., Schöder, H., Yahalom, J., McCall, S. J., Fox, S. Y., Gerecitano, J., Grewal, R., Hamlin, P. A., Horwitz, S., Kobos, R., Kumar, A., Matasar, M., Noy, A., Palomba, M. L., Perales, M.-A., Portlock, C. S., Sauter, C., Shukla, N., Steinherz, P., … Moskowitz, C. H. (2015). PET-adapted sequential salvage therapy with brentuximab vedotin followed by augmented ifosamide, carboplatin, and etoposide for patients with relapsed and refractory Hodgkin's lymphoma: a non-randomised, open-label, single-centre, phase 2 study. The Lancet Oncology, 16(3), 284–292. https://doi.org/10.1016/S1470-2045(15)70013-6
- Pfreundschuh, M. (2017). Age and Sex in Non-Hodgkin Lymphoma Therapy: It's Not All Created Equal, or Is It? American Society of Clinical Oncology Educational Book, (37), 505–511. https://doi.org/10.1200/EDBK_175447
- Radkiewicz, C., Bruchfeld, J. B., Weibull, C. E., Jeppesen, M. L., Frederiksen, H., Lambe, M., Jakobsen, L., El‐Galaly, T. C., Smedby, K. E., & Wästerlid, T. (2023). Sex differences in lymphoma incidence and mortality by subtype: A population‐based study. American Journal of Hematology, 98(1), 23–30. https://doi.org/10.1002/ajh.26744
- Shahid, R., Gulzar, R., Avesi, L., Hassan, S., Danish, F., & Mirza, T. (2016). Immunohistochemical Profile of Hodgkin and Non-Hodgkin Lymphoma. Journal of the College of Physicians and Surgeons--Pakistan : JCPSP, 26(2), 103–107.
- Sureda, A., Arranz, R., Iriondo, A., Carreras, E., Lahuerta, J. J., García-Conde, J., Jarque, I., Caballero, M. D., Ferrà, C., López, A., García-Laraña, J., Cabrera, R., Carrera, D., Ruiz-Romero, M. D., León, A., Rifón, J., Díaz-Mediavilla, J., Mataix, R., Morey, M., … Conde, E. (2001). Autologous Stem-Cell Transplantation for Hodgkin's Disease: Results and Prognostic Factors in 494 Patients From the Grupo Español de Linfomas/Transplante Autólogo de Médula Ósea Spanish Cooperative Group. Journal of Clinical Oncology, 19(5), 1395–1404. https://doi.org/10.1200/JCO.2001.19.5.1395
- Suzuki, K., Terui, Y., Nishimura, N., Mishima, Y., Sakajiri, S., Yokoyama, M., Takahashi, S., Tsuyama, N., Takeuchi, K., & Hatake, K. (2013). Prognostic Value of C-reactive Protein, Lactase Dehydrogenase and Anemia in Recurrent or Refractory Aggressive Lymphoma. Japanese Journal of Clinical Oncology, 43(1), 37–44. https://doi.org/10.1093/jjco/hys194
- Wood, A. J. J., DeVita, V. T., & Hubbard, S. M. (1993). Hodgkin's Disease. New England Journal of Medicine, 328(8), 560–565. https://doi.org/10.1056/NEJM199302253280808
- Zhang, Y., Sanjose, S. D., Bracci, P. M., Morton, L. M., Wang, R., Brennan, P., Hartge, P., Boffetta, P., Becker, N., Maynadie, M., Foretova, L., Cocco, P., Staines, A., Holford, T., Holly, E. A., Nieters, A., Benavente, Y., Bernstein, L., Zahm, S. H., & Zheng, T. (2008). Personal Use of Hair Dye and the Risk of Certain Subtypes of Non-Hodgkin Lymphoma. American Journal of Epidemiology, 167(11), 1321–1331. https://doi.org/10.1093/aje/kwn058
- Zlotnick, M., Avigdor, A., Ribakovsky, E., Nagler, A., & Kedmi, M. (2019). Efficacy of Gemcitabine as Salvage Therapy for Relapsed and Refractory Aggressive Non-Hodgkin Lymphoma. Acta Haematologica, 141(2), 84–90. https://doi.org/10.1159/000495283
Copyright © 2026 by the authors. Licensee Scientific Steps International Publishing Services, Dubai, UAE.
This article is an open access article distributed under the terms and conditions of the
Creative Commons Attribution (CC BY) 4.0 license.