ISSN: 3080-1427 (online) / 3080-1419 (print)
Volume 2, Issue 1 (January 2026 – March 2026), pp: 26-32
![]()
Radical Resection and Deltopectoral Flap Reconstruction Solving the Dilemma of Repeatedly Recurring Submandibular Pleomorphic Adenoma: A Case Report
Shadi Awny 1,a, Sameh Roshdy 1,b, Amany Hassan 2,c, Doaa Khedr 3,d,
Ahmed A Ghanem 4,e, Abdullah N Nassar 1,f, Mohammad Zuhdy 1,5,g*
1 Surgical Oncology Department, Oncology Center, Mansoura University, Mansoura, Egypt.
2 Department of Pathology, Faculty of Medicine, Mansoura University, Mansoura, Egypt.
3 Department of Diagnostic and Interventional Radiology, Mansoura University Hospitals, Mansoura, Egypt.
4 Mansoura University Hospitals, Mansoura, Egypt.
5 Surgical Oncology Department, King Abdullah Medical City, Makkah, Kingdom of Saudi Arabia.
E-mail: Shadiawny@mans.edu.eg a, samehroshdy20@gmail.com b, dramanyhassan@mans.edu.eg c, doaakhedr@mans.edu.eg d,
ahmedghanem9797@gmail.com e, Dr.nassar17@gmail.com f, mzuhdy@mans.edu.eg g,*
Received: 07 July 2025 | Revised: 21 October 2025 | Accepted: 11 December 2025 | Published: 24 January 2026
Pleomorphic adenoma is regarded as the most prevalent salivary gland neoplasm, constituting approximately 80% of all salivary gland tumors. Incomplete surgical resection and/or tumor pseudopodia have been identified as risk factors for recurrence, which can occur despite adequate surgical intervention. The surgical management of recurrence remains challenging, with the complexity of the procedure increasing with subsequent recurrences. With each recurrence, surgical management becomes more challenging. While a considerable number of cases of recurrent parotid pleomorphic adenoma have been documented in the literature, reports of recurrent submandibular gland pleomorphic adenoma are comparatively rare. A 71-year-old female patient with a history of pleomorphic adenoma of the submandibular gland with a seventh recurrence of the malignancy. This recurrence posed significant challenges to the surgical team during the resection process. The patient exhibited 30 years of recurrent symptoms following left submandibular sialadenectomy, with subsequent surgical interventions for management. The surgical intervention involved radical resection, followed by reconstruction of the defect using a tunneled de-epithelialized deltopectoral flap. The patient exhibited a seamless postoperative recovery trajectory, with discharge occurring three days after the procedure. Two years post-surgery, the patient exhibited no evidence of local recurrence. It is hypothesized that radical resection, in conjunction with reconstruction, should be considered a valid surgical intervention to address the surgical dilemma in these cases.
Keywords: Pleomorphic Adenoma; Salivary Gland Tumors; Salivary Neoplasms; Recurrent Pleomorphic Adenoma; Deltopectoral Flap.
According to the findings of Dai et al. (2020), pleomorphic adenoma is regarded as the most prevalent salivary gland neoplasm, constituting approximately 80% of all salivary gland tumors. Surgery is regarded as the primary treatment modality. Enucleation has been the subject of criticism due to its high recurrence rate, which approaches 45%, in contrast to the approximately 3% recurrence rate associated with complete surgical resection (Dulguerov et al., 2017). Incomplete surgical excision or tumor pseudopodia have been posited as potential explanations for recurrence (Steele et al., 2007). Notably, the potential for recurrence persists even following surgical intervention, underscoring the complexity of the condition. The management of this condition is complicated by the fact that subsequent recurrences are observed in approximately 50% of cases. With each recurrence, surgical management becomes more challenging in terms of tumor resection, nerve preservation, recurrence-associated symptoms, and the possibility of transforming into carcinoma ex pleomorphic adenoma (Nicholas et al., 2021). Although numerous cases of recurrent parotid pleomorphic adenoma have been documented in the extant literature, those of recurrent submandibular gland pleomorphic adenoma are comparatively rare (Inan et al., 2016). This phenomenon could be attributed to the enhanced feasibility of complete resection in submandibular sialadenectomy. However, the literature has documented several risk factors for recurrent submandibular pleomeorphic adenoma, including multicentric behavior, the potential for capsule violation during surgery due to proximity to vital neurovascular structures, and the possibility of trapping of epithelial remnants in adjacent lymph nodes (Chauhan & Garg, 2023). In this study, we present a rare case of a seventh-time recurrence of submandibular gland pleomorphic adenoma that represented a challenge in surgical resection.
A seventy-one-year-old female patient was admitted to our department with multiple left-sided cervical swellings. The patient exhibited evident scarring on the affected area, suggesting a history of recurrent disease. The patient exhibited no substantial medical history; however, she had a protracted surgical history, having undergone procedures for the treatment of her submandibular pleomorphic adenoma. The condition manifested initially 30 years ago following a left sialadenectomy for a pleomorphic adenoma. During this period, the patient exhibited an uninterrupted sequence of recurrences, with surgical interventions punctuated by brief periods of disease-free survival, followed by local recurrences. As a result, the patient underwent seven surgical excisions of the cervical pathology. A meticulous pathological examination of all excised specimens revealed a pleomorphic adenoma.
A thorough examination of the patient revealed the presence of multiple, rounded, firm, and non-tender swellings on the left side of the neck, extending from the mandible superiorly to the clavicle inferiorly. The largest of these swellings measured approximately 6 centimeters in diameter and was located in the left posterior neck triangle. The integument over the swellings exhibited an adherent quality. The examination of the facial nerve revealed no significant abnormalities, with the exception of the marginal mandibular branch, which exhibited signs of injury or surgical removal in previous surgical procedures. A thorough examination of the oral cavity revealed no anomalies. With regard to the patient’s medical history, a preliminary diagnosis of a recurring pleomorphic adenoma was proposed (Figure 1(A)).
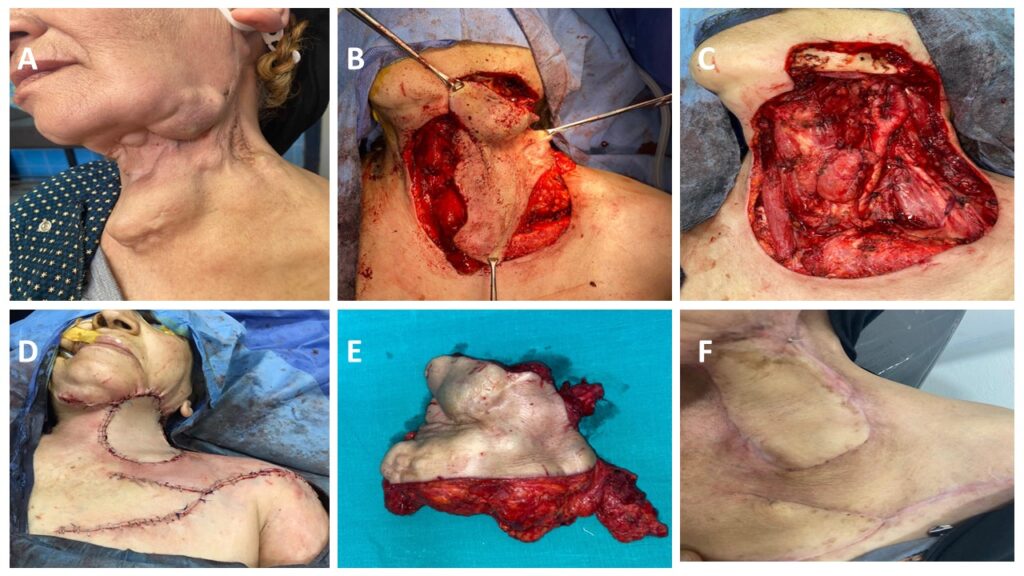
Figure 1. (A): Preoperative Photo Showing Multiple Recurrent Masses at the Operative Bed, (B-D): Intraoperative Photos Showing the Resection of the Multiple Masses Enbloc with the Overlying Skin, the Post-Operative Defect after Resection, and the Reconstruction by the Deltopectoral Flap Respectively, (E): Intraoperative Photo of the Operative Specimen, (F): A 2-Year-Follow Up- Photo of the Patient
A comprehensive head and neck evaluation was conducted using magnetic resonance imaging (MRI), which revealed multiple variable-sized masses of mixed signal intensities on the left side of the neck. The involvement of the left submental and submandibular regions, masticator space, mandibular angle, posterior auricular area, posterior triangle, and carotid spaces were observed. These masses were inseparable from the left parotid tail. The presence of mixed SI on T1 and T2 WI was observed, indicating an underlying hemorrhagic component with heterogeneous enhancement on post-contrast imaging. The most substantial lesion was observed in the left posterior triangle, with dimensions measuring 3.7×4.7 centimeters. A few tiny reactive right submandibular and jugular nodes were detected (Figure 2(A,B)).
Computerized tomography (CT) revealed multiple heterogeneous enhancing soft tissue lesions involving left-sided neck spaces that were previously mentioned in the MRI report. The remaining findings of the study were deemed irrelevant with the exception of bilateral pulmonary nodules, with the largest measuring 10 millimeters (Figure 2(C)). This multicentric recurrent behavior raised an alert for the need for more radical resection and possible reconstructive procedure. A core needle biopsy was performed on one of the left-sided neck swellings, confirming the diagnosis of recurrent PMA.
A multidisciplinary team discussion (MDT) with patient counseling resulted in a consensus to alter the surgical strategy, deviating from the conventional approach of skin incision and localized excision of the recurrent masses, which had proven to be ineffective in halting the persistent recurrences. A comprehensive excision of all lesions was meticulously planned en bloc with the overlying skin, with the objective of preventing the recurrence of the observed pathology. In the absence of the challenging resection, the reconstruction of the expected substantial neck defect proved to be more arduous due to the vessel-depleted neck and the patient’s poor general condition.
The patient underwent a radical resection that included the skin, prevertebral muscles, and the lesions en bloc with the overlying skin, sternomastoid muscle, and internal jugular vein. The substantial neck defect was reconstructed using a tunneled, de-epithelized deltopectoral flap, with the flap donor site primarily closed (Figures 1(B-D)). The operative time was five hours, with minimal blood loss. The patient exhibited a uneventful postoperative recovery and was discharged from the hospital three days after the procedure. Following a period of ten days, the flap demonstrated signs of viability, and the sutures were removed.
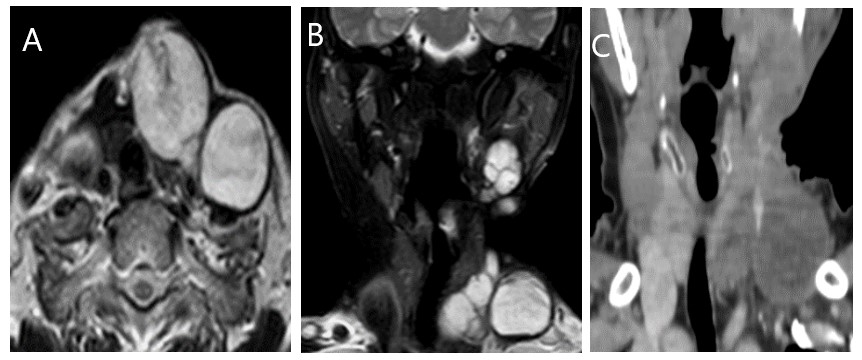
Figure 2. MR and Post-Contrast CT Examination of the Patient Revealed: (A) Axial T2 Lobulated Lesion at the Left Supraclavicular Region with Hypointense Rim Wall Compressing Related Vessels Posteriorly. (B) Coronal SPAIR MR, Shows Multiple Lesions Seen at the Left Side of the Neck Submandibular and Left Supraclavicular Region. (C) Post-Contrast Coronal CT Show Mildly Enhancing Lesions at the Left Supraclavicular Region Encasing the Left Internal Jugular Vein.
The excised specimen measured approximately 13×16 centimeters (cm) (Figure 1(E)). It was covered by a skin ellipse. A meticulous pathological evaluation of the specimen revealed the presence of lobulated masses that occupied a significant portion of the specimen. These masses were accompanied by cystic areas, characterized by hemorrhage and friable content, alternating with solid, firm, grayish-white areas. Microscopic examination revealed the presence of benign tumoral proliferation, which manifested as nodules comprising three distinct cell types: ductal epithelial cells, spindled stromal component, and epithelioid myoepithelial cells, situated within a myxoid background. The epithelial cells are characterized by an eosinophilic cytoplasm and round nuclei that appear unremarkable. Myoepithelial cells are present, as are bland spindled, epithelioid cells, which exhibit areas of hemorrhage. The final diagnosis was recurrent Pleomorphic adenoma (Figure 3). Two years post-surgery, the patient exhibited no evidence of local recurrence, as illustrated in Figure 1 (F).
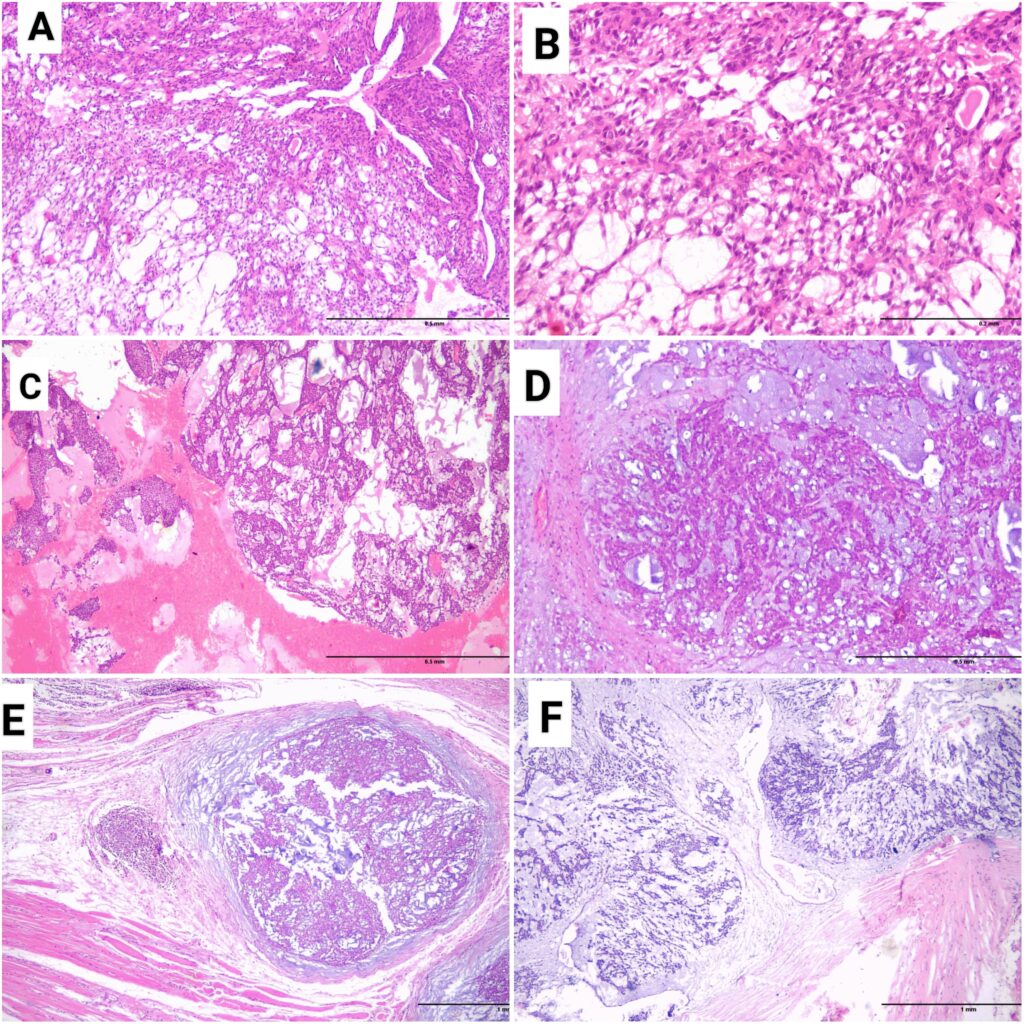
Figure 3. (A&B): Microscopic Picture of the Primary Tumor Showed the Biphasic Appearance with Epithelial, Myoepithelial, and Stromal Components (H&E, x40 & x200 Respectively). (C-F): Images from the First, the Third, the Fourth, and the Last Recurrences Respectively (H&E, x40, x200, x40 & x40 Respectively).
The majority of salivary gland neoplasms are benign, while malignant neoplasms constitute approximately 14% of these lesions. The most prevalent salivary gland tumor is pleomorphic adenoma, which accounts for more than 70% of all salivary gland tumors (Valstar et al., 2017). Complete surgical resection is regarded as the standard of care for this condition, with a documented 5% recurrence rate (Nicholas et al., 2021).
The patient exhibited symptoms consistent with recurrent and metastasizing pleomorphic adenoma, including multiple masses in the head and neck region, cranial nerve affection, abdominal masses, spinal cord compression, and nasal obstruction. Metastasizing pleomorphic adenoma is an infrequent subject in the medical literature, with a mortality rate of 22%. Local recurrence was observed to precede metastasis in approximately 80% of cases (Sedat et al., 2015). According to the World Health Organization, this tumor is histologically benign but with the possibility of distant or local metastasis, even to the head and neck region and regional lymph nodes (Nouraei et al., 2006). The following report details a case of recurrent pleomorphic adenoma of the submandibular gland. The patient underwent their initial surgical intervention in 1987 at a facility external to our center. This was followed by seven subsequent recurrences, which were addressed through a comprehensive resection and reconstruction procedure involving the deltopectoral flap.
Despite the existence of numerous studies in the literature that have explored the potential causes of pleomorphic adenoma recurrence, the precise underlying factors remain to be elucidated. The primary hypothesis centered on the incomplete surgical resection of the tumor, a phenomenon that might be attributed to one of two possible factors. Firstly, surgical factors, such as inadequate surgical resection techniques (e.g., enucleation), insufficient margins due to proximity to nerve branches, tumor rupture, or spillage, could be responsible. Secondly, pathology-related factors, including deficient capsule, tumor satellite nodules, pseudopodia, multicentricity, and a high Ki67 index (Dai et al., 2020; Dulguerov et al., 2017), could be implicated.
Recurrent pleomorphic adenoma of the submandibular gland is a rare and challenging condition (Inan et al., 2016). In their study, Abdallah et al. reported recurrent pleomorphic adenoma of the submandibular gland to represent approximately 20% of all recurrent pleomorphic adenomas (Abdallah et al., 2025). In their case report, Inan et al. documented a 32-year-old female patient who experienced recurrence five years after excision. The surgical intervention involved the excision of the mass, accompanied by level I, II, and III cervical lymph node dissection. In the course of a 1-year follow-up period, no reoccurrence of the phenomenon was observed (Inan et al., 2016). Li et al. reported on a 28-year-old patient who presented with a recurrent right submandibular mass, 10 years after its previous excision. The surgical intervention involved a right submandibular gland and mass resection, accompanied by cervical lymph node dissection and the use of an arbitrary skin flap. However, the absence of any subsequent follow-up on the case is a notable lacuna in the research, as pointed out by Li et al. (2025).
In a separate report, Chauhan and Garg documented a 22-year-old case of recurrent left submandibular pleomorphic adenoma following prior resection approximately a decade prior. During the surgical procedure, two tumor nodules and the scar tissue were resected from the operative bed. The patient did not report any recurrence of the disease over a period of six months (Chauhan & Garg, 2023).
Carcinoma ex pleomorphic adenoma signifies a malignant transformation of pleomorphic adenoma of the salivary gland. According to Ghaloo et al. (2022), the incidence of malignant transformation has been documented to be 1.5% following a period of five years from the initial diagnosis, and 3.3% in cases of recurrence. The occurrence of malignant transformation in recurrent pleomorphic adenoma has been documented in 1.5-23% of cases, with this risk increasing with time and the number of recurrences. Furthermore, a more unfavorable prognosis for carcinoma ex recurrent pleomorphic adenomas was also reported (Mariano et al., 2016).
The patient’s medical history included a prior submandibular sialoadenectomy in 1983, followed by surgical interventions for recurrences in 1987 and 2017 at external medical centers. Subsequent to this initial presentation, the patient was admitted to our medical center in 2018 with the fourth recurrence of the disease. There, she underwent a procedure known as resection, in which multiple recurrent tumor nodules were removed. This procedure was repeated until the final recurrence in 2021. It is noteworthy that the radical resection of the multiple tumor nodules, in conjunction with the overlying skin and fascia, was meticulously executed. A deltopectoral flap was utilized for the reconstruction of the skin defect. In their study, Aro et al. reported an incidence of recurrent submandibular gland pleomorphic adenoma in six patients, with only one patient experiencing seven recurrences. The recurrence pattern was documented as multifocal in 57% of patients. Furthermore, they discovered that the interval between successive occurrences decreased progressively until the subsequent recurrence was observed (Aro et al., 2019).
The deltopectoral or Bakamjian flap is regarded as a highly versatile flap, frequently utilized in the reconstruction of defects that arise subsequent to head and neck surgeries (Chan & Chan, 2014). The material’s thin and pliable nature ensures a precise color and texture match. In addition to this, the harvesting process has been shown to be both safe and straightforward (Mikami et al., 2017). In this particular case, a deltopectoral flap was utilized to cover the defect subsequent to radical resection of all recurrent tumor nodules and overlying skin and fascia, yielding satisfactory cosmetic and functional outcomes. Given the vessel-depleted neck, the patient’s poor general condition, and the unpredictable prognosis of the tumor, a pedicled flap was preferred over a free tissue transfer. The pectoralis major myocutaneous flap was selected as the final recourse.
While there have been multiple documented cases of recurrent parotid pleomorphic adenoma, cases of recurrent adenomas of the submandibular gland are less frequently reported. The pattern of recurrence with multifocal tumor nodules poses a significant surgical challenge. It is hypothesized that radical resection, in conjunction with reconstruction, should be considered a valid surgical intervention for cases presenting such a surgical dilemma. It is important to note that this option has been shown to yield superior oncologic outcomes by facilitating more radical resection and decreasing the probability of recurrence. Furthermore, it yielded superior cosmetic and functional outcomes, thereby enhancing the patient’s quality of life.
Ethical approval is not required for this study in accordance with Egyptian national guidelines. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Not applicable.
No new data was generated or analyzed in this study.
The authors declare that there are no conflicts of interest.
The authors declare that this research received no external funding.
S.A: Conceptualization, Writing – review & editing.
S.R: Conceptualization, Writing of the original draft, Supervision.
A.H: Investigation, Data curation.
D.K: Investigation, Data curation.
A.A.G: Data curation, Writing – review & editing.
A.N.N: Data curation, Writing – review & editing.
M.Z: Data curation, Writing of the original draft, Writing – review & editing.
Not applicable
The authors declare that no generative AI or AI-assisted technologies were used in the preparation of this work.
Cite: Awny, S., Roshdy, S., Hassan, A., Khedr, D., Ghanem, A. A., Nassar, A. N., & Zuhdy, M. (2026). Radical Resection and Deltopectoral Flap Reconstruction Solving the Dilemma of Repeatedly Recurring Submandibular Pleomorphic Adenoma: A Case Report. Middle Eastern Cancer and Oncology Journal, 2(1), 26-32. https://doi.org/10.61706/MECOJ160204


An independent academic publisher with an editorial team including many of the top researchers in the world. SSG publishes research, review, and case report articles in double-blind, peer-reviewed, open access scientific and academic journals.
Copyright © 2025 Scientific Steps International Publishing Services LLC (Dubai – United Arab Emirates)